
|
|
Colonization
Historical Trauma
Racism
Helplines
Creative Processing
Poetry
Episode Transcripts
White Supremacy Culture
Other Important Links
Colonization
Colonization
Colonization is an ongoing process which forces people off of their native lands and forces them to live under an external, foreign set of rules, laws, and beliefs. All of the United States is colonized. There are many good resources for understanding how this affects everyone.
The Alaska Native Tribal Health Consortium offers a free participatory history lesson called the Alaska Blanket Exercise that helps people in Alaska understand the effects of colonization. Find out more here and listen to the first half of the episode with Jackie Engebretson.
Native Movement is a nonprofit based in Alaska that offers classes on understanding settler colonialism and its lasting effects. They also have a resource page with podcasts, books, articles, and more.
Native Lands is a world map that shows who are the Indigenous people in many parts of the world. Find out whose land you are on then learn more.
If you have other good resources to share, please email Anne at [email protected].
The Alaska Native Tribal Health Consortium offers a free participatory history lesson called the Alaska Blanket Exercise that helps people in Alaska understand the effects of colonization. Find out more here and listen to the first half of the episode with Jackie Engebretson.
Native Movement is a nonprofit based in Alaska that offers classes on understanding settler colonialism and its lasting effects. They also have a resource page with podcasts, books, articles, and more.
Native Lands is a world map that shows who are the Indigenous people in many parts of the world. Find out whose land you are on then learn more.
If you have other good resources to share, please email Anne at [email protected].
Historical Trauma
Historical Trauma
Historical trauma is the idea that trauma, such as forced displacement or war, can affect the health of multiple generations not just the ones that experienced the trauma first-hand. The trauma is perpetuated and aggravated by systems of oppression. There's extensive academic research around the lasting effects of historical trauma by both Indigenous and non-indigenous authors. It's also been covered by numerous popular media outlets.
Here are a few links to some useful resources:
Here are a few links to some useful resources:
Collective understanding
Dr. Joseph Gone, a member of the Aaniiih-Gros Ventre tribal nation in Montana and a psychiatrist at Harvard University, writes a lot about historical trauma and healing justice in Indigenous communities. You can read more about his work here.
In a 2019 interview with Mad in America, which is worth a full listen, he said:
Dr. Joseph Gone, a member of the Aaniiih-Gros Ventre tribal nation in Montana and a psychiatrist at Harvard University, writes a lot about historical trauma and healing justice in Indigenous communities. You can read more about his work here.
In a 2019 interview with Mad in America, which is worth a full listen, he said:
|
Historical trauma "recognizes our problems today but anchors their origin in our histories of oppression so we can get out of the paralyzing self-blame narratives. We have to re-socialize a series of issues that have been medicalized for a long time, which in turn has led to individuation where only the individual is the site of therapeutic engagement. With historical trauma, it is about entire communities that have been deliberately impoverished and are in need of desperate remedies. This may look less like healing and more like justice."
|
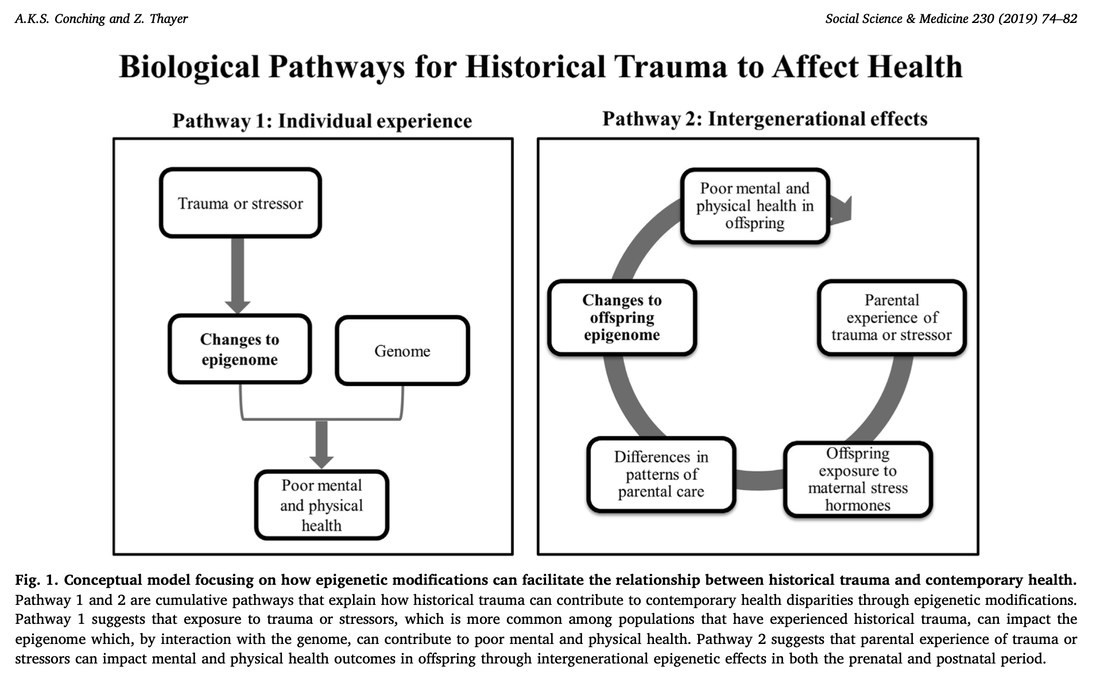
A model to understand the biological effects of historical trauma
Andie Kealohi Sato Conching and Zaneta Thayer wrote a piece in Social Science and Medicine in 2019 that puts forth two different biological pathways for historical trauma to affect the health of multiple generations. The example they provide of a pregnant Native Hawaiian woman in 1848, when Native Hawaiians lost rights to their land, makes it much easier to understand. Here's the full text.
Andie Kealohi Sato Conching and Zaneta Thayer wrote a piece in Social Science and Medicine in 2019 that puts forth two different biological pathways for historical trauma to affect the health of multiple generations. The example they provide of a pregnant Native Hawaiian woman in 1848, when Native Hawaiians lost rights to their land, makes it much easier to understand. Here's the full text.
Healing from historical trauma
This article by Natalie Avalos, PhD explains both colonization and historical trauma and offers a path forward for healing. She writes, "historical trauma has been described as a soul wound because it is experienced as a wounding down to the level of being...it is instigated by a total loss of lifeways, producing deep philosophical disorientation."
Healing requires restoring "healthy relationships to one’s self and members of the larger social body," she writes. "This social body includes the natural world and all living within it, human and other-than-human, such as plants and animals, but also one’s ancestors."
BBC: Can the legacy of trauma be passed down the generations?
This 2019 BBC article gets into details about epigenetics in a pretty accessible way starting with a look at U.S. Civil War veterans. The author details studies done on mice as well as with humans in a way to explore the biological process. Read the full article here.
This article by Natalie Avalos, PhD explains both colonization and historical trauma and offers a path forward for healing. She writes, "historical trauma has been described as a soul wound because it is experienced as a wounding down to the level of being...it is instigated by a total loss of lifeways, producing deep philosophical disorientation."
Healing requires restoring "healthy relationships to one’s self and members of the larger social body," she writes. "This social body includes the natural world and all living within it, human and other-than-human, such as plants and animals, but also one’s ancestors."
BBC: Can the legacy of trauma be passed down the generations?
This 2019 BBC article gets into details about epigenetics in a pretty accessible way starting with a look at U.S. Civil War veterans. The author details studies done on mice as well as with humans in a way to explore the biological process. Read the full article here.
Racism
Racism and mental health
Structural racism in mental health treatment: Oppression and structural racism have a direct impact on mental health, and the mental health system is itself racist and classist. The diagnoses and medications people receive are in part determined by their race and class. Dr. Helena Hansen provides personal examples and delves into her research during this 2021 interview with Mad in America. Listen to it or read the transcript.
Social determinants of mental health: Our mental health is affected by more than just the chemicals in our brains and personal experiences. It's also shaped by the environment around us and our access to resources like food, education, housing, green space, etc. Dr. Ruth Shim talks about this during the episode on racism and mental health. Learn more about her work here and here. Or if you'd rather listen to her speak more, check out her talks on YouTube or check out her interview (and others!) at Unapologetically Black Unicorns.
Looking for books on these topics? Check out The Protest Psychosis by Jonathan Metzl or (Mis)Diagnosed: How Bias Distorts our Perception of Mental Health by Jonathan Foiles.
Social determinants of mental health: Our mental health is affected by more than just the chemicals in our brains and personal experiences. It's also shaped by the environment around us and our access to resources like food, education, housing, green space, etc. Dr. Ruth Shim talks about this during the episode on racism and mental health. Learn more about her work here and here. Or if you'd rather listen to her speak more, check out her talks on YouTube or check out her interview (and others!) at Unapologetically Black Unicorns.
Looking for books on these topics? Check out The Protest Psychosis by Jonathan Metzl or (Mis)Diagnosed: How Bias Distorts our Perception of Mental Health by Jonathan Foiles.
Helplines
Who to call for help
National Suicide Prevention Lifeline - 1-800-273-8255 -- Available 24/7/365
Careline Alaska - 1-877-266-4357 (HELP) -- Available 24/7/365
NAMI (National Alliance on Mental Illness) - Find your local chapter here.
SAMHSA’s National Helpline - 1-800-662-4357 -- For substance misuse treatment referrals
Lines for Life - This service is based in Oregon and offers helplines for specific groups:
Careline Alaska - 1-877-266-4357 (HELP) -- Available 24/7/365
NAMI (National Alliance on Mental Illness) - Find your local chapter here.
SAMHSA’s National Helpline - 1-800-662-4357 -- For substance misuse treatment referrals
Lines for Life - This service is based in Oregon and offers helplines for specific groups:
- Racial Equity Support Line - 503-575-3764
- Military
- Call 888-457-4838 (24/7/365)
Text MIL1 to 839863 Monday-Friday, 2-6pm PT
- Call 888-457-4838 (24/7/365)
- Teens - Talk to teen peer support from 4 - 10 pm PT, adults at other hours
- Call 877-968-8491
Text teen2teen to 839863
- Call 877-968-8491
Creative Processing
Creative processing
We are all affected by colonization, historical trauma, and systemic oppression and inequities. We cannot disconnect ourselves from the past, present, and future of the lands where we live. And all of that can be a lot to process.
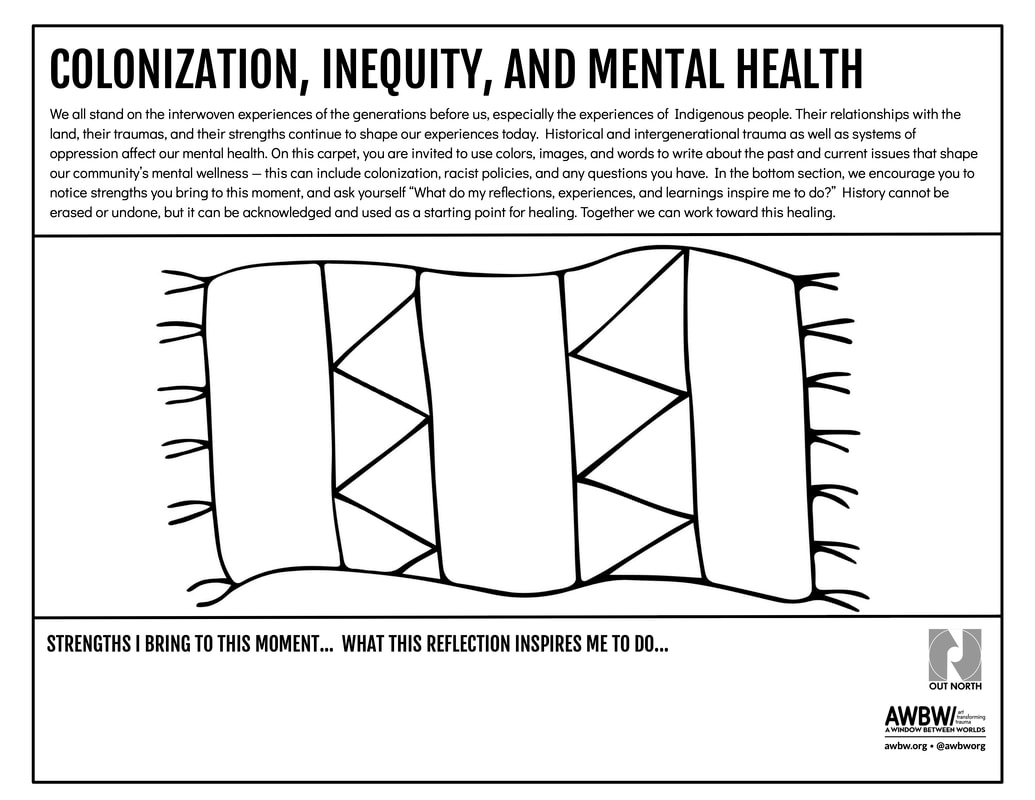
For this exercise you can use any supplies you have, from a scrap of paper and a pen to paints and pastels. You can also download the worksheet below. Using words or images, write down the long-term community factors that affect mental health. This may include effects of colonization or racist policies. Write down any questions you may have, too. You may want to ground yourself before doing this exercise by taking a few deep breaths while thinking about your community’s history.
When you finish, you may want to crush up the paper and throw it or stomp on it. These issues are very emotional and safe physical releases are healthy. Or you may choose to post it somewhere as a reminder of what we need to heal from.
History cannot be undone, but we can acknowledge it and move forward with a focus on equity and healing.
For this exercise you can use any supplies you have, from a scrap of paper and a pen to paints and pastels. You can also download the worksheet below. Using words or images, write down the long-term community factors that affect mental health. This may include effects of colonization or racist policies. Write down any questions you may have, too. You may want to ground yourself before doing this exercise by taking a few deep breaths while thinking about your community’s history.
When you finish, you may want to crush up the paper and throw it or stomp on it. These issues are very emotional and safe physical releases are healthy. Or you may choose to post it somewhere as a reminder of what we need to heal from.
History cannot be undone, but we can acknowledge it and move forward with a focus on equity and healing.
Poetry
Poetry
No Justice George No Peace Breonna (2020)
by M.C. MoHagani Magnetek
Where are you now that George Floyd has died
Are you down and ready to ride
Take no more with your last breath
Let the system burn till there’s nothing left
But the hardcore reality that black lives matter
Water cooler convo filled with chatter
Calling into question your humanity
Like a grudge, Corona got a grip on sanity
Got folks sick tired hot bothered and sad
Everybody and their mama all pissed-off and mad
About a black woman shot and killed in her own house
Don’t act like you don’t know Breonna Taylor is who I’m talking about
So yeah don’t worry about that bucket of water
Remember the centuries of genocide and slaughter
Superiority complex can’t be unlearned
And so what… the roof is on fire. Let it burn
Give them no choice
But to listen and respect our voice
Get your hands out my pockets!
No Means No We Said Stop It!
Murderers getting paid on administrative leave
Promoted for using their knees
To choke hope out of the ppl
All lives matter, C’mon mayne… this shit ain’t equal
Tell me what’s making a difference supposed to look like
Match struck fireworks in broad daylight
No longer satiated
Refused to be placated
Until the killing of our people cease
If there’s no Justice for George & Breonna, there will be no PEACE.
by M.C. MoHagani Magnetek
Where are you now that George Floyd has died
Are you down and ready to ride
Take no more with your last breath
Let the system burn till there’s nothing left
But the hardcore reality that black lives matter
Water cooler convo filled with chatter
Calling into question your humanity
Like a grudge, Corona got a grip on sanity
Got folks sick tired hot bothered and sad
Everybody and their mama all pissed-off and mad
About a black woman shot and killed in her own house
Don’t act like you don’t know Breonna Taylor is who I’m talking about
So yeah don’t worry about that bucket of water
Remember the centuries of genocide and slaughter
Superiority complex can’t be unlearned
And so what… the roof is on fire. Let it burn
Give them no choice
But to listen and respect our voice
Get your hands out my pockets!
No Means No We Said Stop It!
Murderers getting paid on administrative leave
Promoted for using their knees
To choke hope out of the ppl
All lives matter, C’mon mayne… this shit ain’t equal
Tell me what’s making a difference supposed to look like
Match struck fireworks in broad daylight
No longer satiated
Refused to be placated
Until the killing of our people cease
If there’s no Justice for George & Breonna, there will be no PEACE.
Episode Transcripts
Colonization & Oppression
Ways to Decolonize
Racism
Colonization & Oppression
Colonization and Oppression - Part One
[00:00:00] Anne: Welcome to Mental Health Mosaics, an exploration of mental health from Out North, which is located on the unceded traditional lands of the Dena'ina People in Anchorage, Alaska. I'm Anne Hillman.
When we talk about mental health we often focus on what's happening to each of us as individuals and how we're dealing with life right now. But humans don't exist in bubbles. What happened in our community's past and what's currently happening, including racism and inequity, affects all of us and our mental health. We can't ignore it. So for the next two episodes we're going to focus on colonization, white supremacist culture, and mental health. Yes -- this is going to be heavy and yes, you are probably going to be uncomfortable.
This episode is kind of a primer -- we'll jump into the basics of how colonization in Alaska is having a long-term impact on mental health, why teaching that history is so important, and have a more philosophical conversation about understanding what historical trauma is.
If you are well-versed in Alaska Native history and understand, especially through personal experience, the effects of intentional cultural destruction, this episode is full of triggers and you may want to skip it. But we don't just talk about trauma, we also talk about strength because every culture and every community has both. If you are a non-Indigenous person, especially one who lives in Alaska, please keep listening. This is just the start of what we all need to know when living on Indigenous lands whether you care about mental health or not. So, without further ado, please meet Jackie, who was willing to provide a pretty intense history lesson.
[00:01:50] Jackie: My name is Jackie Engebretson and my family is from Gulkana, which is in the Copper River region here in Alaska and I'm Ahtna Athabaskan, although I grew up in both Copper Center and Valdez. Currently, I am a senior program manager in the behavioral health department at the Alaska Native Tribal Health Consortium.
[00:02:09] Anne: Well, thank you so much for joining us today. So I'd love to start with conization. What does that mean? And what does that mean in Alaska context?
[00:02:18] Jackie: Colonization would be when an outside country/entity comes into another space and takes over in a sense. They start occupying the land as if it was their own. They start making their own rules and laws as if they were the like supreme leaders of that space. Most often that means they are supplanting local populations. So in the state of Alaska there've been many different colonizing forces. Initially the colonizers would be the Russians, particularly in a Western Alaska and in the Aleutians.
Other areas of Alaska did not have as much of a Russian influence, so they had people like missionaries come in, people like the U. S. army come in, and those were their primary colonizers.
So in those instances, like been particularly areas that were colonized by Russians, you saw Russian orthodoxy takeover. You saw Russian culture, Russian language become more predominant. And then in areas where Christian missionaries came in. You saw Christian churches, Christian schools, and rules centered around Christianity instead of the local indigenous populations.
[00:03:38] Anne: And instead of around local and Indigenous belief systems?
[00:03:40] Jackie: Correct, yes.
[00:03:42] Anne: Why is that damaging?
[00:03:45] Jackie: So you have a group of people in the state of Alaska, that'd be Alaska Nativesm who have occupied the land for tens of thousands of years. And they have used the land in ways that feed their family, that nourish their soul, and it's their home.
And all of a sudden you have these people coming in who have a different viewpoint when it comes to how you use land. With Russians, they did a lot of trapping and hunting and over trapped and over hunted resources that Alaska Native people have been using for many, many years without impacting the animal populations.
Resources that were once available are no longer available. You have people occupying spaces that were historically yours. That could be places where your family used to gather food. That could be places where your family used to go to practice spiritual practices. That could be places where your family has just traditionally occupied and all of a sudden there are Russians or Americans living in this land and telling you that you can no longer use it. And it can impact the way you hunt and just it impacts all ranges of your life.
[00:05:03] Anne: And does it impact mental health?
[00:05:05] Jackie: Yes, it can absolutely impact mental health. That's some of the things that we see more long-term here in Alaska.
Particularly as colonization continues. There's like restrictions on how you can hunt, when you can hunt, who else is allowed to hunt, and who else is on your land. They're telling you what you must believe. When your whole way of life is just shifted that way, you lose many different protective factors. And so protective factors are things that kind of keep you mentally and physically safe. So with Alaska Native people -- with people in general, to be honest, this is not just a Native thing -- but identity is a huge part of what helps people feel more rooted in who they are.
And in the United States, there is a general lack of identity, not just with Alaska Native people, not just with Indigenous people. There are a large number of people in this country who just don't have that sense of identity that maybe previous generations would have or maybe other groups throughout the world do have.
[00:06:11] Anne: Just because in the United States, there's is this giant push towards assimilation, and we are all the same, and there is a dominant culture and, and it sort of eliminates our roots and our connections.
[00:06:23] Jackie: Absolutely. And so that's especially true here in Alaska with Alaska Native people. The long-term impacts of colonization might include things like I mentioned, not being able to hunt. So for a lot of Alaska Native men, for instance they had roles that they were expected to fulfill including hunting and gathering and things like that. And now those roles are limited and they no longer have the same ability to do things that they might have previously.
Historically, my people were semi-nomadic so they would move from camp to camp depending on the season. They'd have fish camp and they'd have a hunting camp and they'd have places they'd go to pick berries and things like that. And that was down to the family level.
But after colonization, there was a huge push for families to stay in one spot so that the kids could go to school. “This is in the best interest of your kids. And if you want them to have a good education and a good life, then you need to stay here in this village and your kids need to go to school. They need to go to school following this schedule and that schedule doesn't follow subsistence hunting.
It doesn't follow it -- doesn't follow anything. It follows this arbitrary date that the U.S. government or the state government has told kids that they must be in school. So things like that. You're not following your own traditional and cultural practice. Instead, you're doing what is expected of you by the U.S. government.
[00:07:52] Anne: And at the same time, there's still a practical need to hunt and gather in rural Alaska to get the food and nutrition people need to survive.
[00:08:02] Jackie: We know what naturally grows in Alaska and how we receive our nutrients. You know, traditional Alaska Native diets fulfilled all the nutritional needs. And without eating all of those foods, you're not getting the same needs and instead you need to supplement them with things that you might get from the grocery store. And the items that you might get to supplement your nutritional needs from the grocery store might be extremely expensive because it needs to be shipped up from the United States.
You might have to take vitamins and things like that. So I think from a practical purpose, it's something that's still necessary today. There’s a nutritional basis. And then just the spiritual connectedness that comes from hunting and gathering and being connected to the land and being part of and having a relationship with the land that you have for tens of thousands of years is also still important.
[00:08:56] Anne: And that, again, brings us back to mental health and how these spiritual connections keep us well. I mean, physically well, but also well as whole people. You mentioned earlier, it's not just restrictions on land. Just limiting of land use and movement that happened through colonization, but you also mentioned that churches and missionaries came in.
How did that affect the Indigenous peoples of Alaska?
[00:09:30] Jackie: Yeah, I think the most notable example and one that's probably most relevant to the discussion today would be boarding schools. So throughout the state there were -- and this is honestly something that's an international thing is not something that just happened here in Alaska. We've seen a lot of talk about it in the news recently, due to mass graves being uncovered in Canada. Mass unmarked graves from children in Canada, children that were never returned home.
So the boarding schools were set up to assimilate Indigenous youth. And there was this mentality at the time where the idea was to “save the man and kill the Indian.”
So you save the man by sending them to school, to this boarding school, away from their family, away from their community. And you kill the Indian by not allowing them to speak their language, by not allowing them to be raised by their community and not practice their spiritual practices, their traditional practices, not allowing them to sing their songs, not allowing them to dance.
And by the time you're done with them with them, by the time they were done with boarding school, if they survived, they would be sent back to their communities and no longer feel a sense of identity. Or feel very disconnected from their identity. Not only from their identity, but from their family, from their mom, their dad, from their community.
And many people who go into boarding school just never returned to their community, whether it be because they passed away or because they just no longer felt like they were a part of their community. One of the ways that they would assimilate was by not allowing them to speak their language and children would be punished.
I've heard many stories from elders and I think a lot of other people have heard other stories as well. Punishment, like restricting food, not allowing them to eat. Physical punishment, whether it be spanking, beating, a lot of really terrible, terrible things happened to children in boarding schools.
[00:11:33] Anne: And just a side note here -- the boarding schools in Alaska were started by missionaries. By the early 20th century, they were run by the federal government. It was the U.S. government's policy to take children away from their families and sometimes send them to the other side of the continent. And all of this led to really negative long-term consequences that we still feel today. This isn't just a history lesson. Boarding schools have created persistent, intergenerational trauma. Back to Jackie.
[00:12:06] Jackie: Because they weren't raised by their families, a lot of youth who went through boarding schools didn't have a model of what parenting should look like. So when they grew up to be adults, they had hard time parenting themselves.
They might not have been the healthiest parents. They might not have been the most present parents. It had a lot of long-term impacts on parenting. It had a lot of long-term impacts on people's mental health and their physical health. We know that when people experience Adverse Childhood Experiences that there's long-term impacts to that. It could affect your physical health. It's higher rates of diabetes, higher rates of obesity. It can impact their mental health. They're more likely to interact with the criminal justice system. All of those, I mean like many more things as well.
[00:12:56] Anne: Use substances?
[00:12:57] Jackie: Use substances. Exactly. Exactly. Substance use rates are also very, very high for people who have high ACE scores. Going to a boarding school is just a number of ACEs that add on, with an added aspect of like racism in it as well.
[00:13:16] Anne: Talk more about the aspect of racism. I mean the obvious eliminate who you are and eliminate cultures.
[00:13:24] Jackie: Yeah. So all of this was rooted in the idea, like I mentioned of kill the Indian, save the man. So the idea is that since colonization here in the United States and worldwide as well, is that people of non-European descent are lesser than. They're like lesser than human often, but they're certainly lesser than their white counterparts. So there was this idea that American Indians and Alaska Natives and other populations worldwide were savage or that they were uncivilized or that they were backwards.
And just this idea that they were not equal and that they needed to change. And that colonization was to save them and was a good thing for them. And that European people were supreme and were just more civilized and therefore were doing you a favor. So there was a racial component in the boarding schools because they wanted Native youth to be more like white people.
[00:14:31] Anne: Thinking about this intentional move to cut people off from their families, to cut people off from their culture, to try to make them into someone else. I feel like that hasn't stopped to this day, so how does that relate to behavioral health? Like why do you as a behavioral health organization work to make sure that people understand the complexities of these issues?
[00:15:02] Jackie: That's a great question. I can use myself as an example if that helps.
The reason why this kind of work is really important to me is because of my own kind of lived experiences and things that I've seen in my family, friends, my community. But talking about me specifically since it's my story and my place to tell. I grew up in a very complicated family system. And I know that we all loved each other, but there was trauma that was carried over through generations.
My parents experienced trauma from their parents and my grandparents experienced trauma from their parents. I honestly don't know how far back it goes, but I would imagine it goes back pretty far.
And I think some of it is rooted in some of the things that happen to our community and perhaps how people were treated many, many generations ago that still shows up today. And so I grew up thinking that there was something wrong with me, thinking that there was something wrong with my family and that there was something wrong with my community. Some of the challenges that I had in my own life -- I struggled with depression. I still do. And then eventually I struggled with substance use, and I thought that was because I was Native. And I thought it was because there was something wrong with my family. And I thought that it was just kind of my destiny and like it was going to happen. And it was inevitable.
[00:16:28] Anne: Just because you were Native?
[00:16:30] Jackie: Yeah, because the messages I received, I think from everybody. Everybody gave you these messages. Um, certainly when I was in school, I was a high achiever. I didn't have a lot of Native friends when I was in high school. And I would hear people say things about Natives and I'd be like, “Oh, they're not talking about me though.”
It like took until I had become an adult to really understand. It's like, well, even if they weren't talking about me, they were definitely talking about some of my cousins. Or they're definitely talking about my auntie or my uncle. So yes, they were talking about me, and I just thought I was like one of the good ones when I was in high school or something. And then I had this like crashing reality when I was on my own and an adult and trying to just deal with all these complicated things that I had experienced in life and wondering what's wrong with me. And I know that this is true for other people all over the place.
And I know that there are still people who are living in these really complicated patterns in their life because of historical trauma, because of intergenerational trauma. Who are internalizing that and thinking that there's something wrong with them or maybe thinking that there's something wrong with everybody around them. And not understanding that there's been a lot of things that have happened to us as a people, as family systems that are just really difficult to overcome. And unless you have access to resources and unless you're aware of what's going on, you're not going to be able to get the help. You're not going to, or you might not even want to. And if you think that there's something wrong with you, you're going to think there's probably something wrong with going to therapy or there's probably something wrong with going to treatment. Or there's something wrong with taking medications that can help manage your mental health.
So there's like all these really complex thought processes that go on with people. And the added like racism and stigma associated with a lot of the things we talked about, substance use, mental health, being involved in the criminal justice system, that just like all these different barriers that make people not want to access care.
So the reason why we at ANTHC decided to share the Alaska Blanket Exercise widely is because we wanted providers to understand, “Hey, your patient, isn't just not showing up or like not taking their medication because they don't want to, or because they're willfully being ignorant they're willfully being bad patients. It's because they have a lot of things going on in their lives and they're doing the best that they can to show up. And you need to understand this. You need to understand their traumas.”
It's to help Alaska Native people understand, "Hey, this is, this might be why your family is the way that they are, and there's nothing wrong with you. It's just, there's, there's been a lot that has happened." It think it just helps people be more compassionate for others and for themselves.
[00:19:33] Anne: Explain what this Blanket Exercise is.
[00:19:40] Jackie: Sure. So the Alaska Blanket Exercise is a participatory history lesson. We initially partnered with a Canadian organization called Kairos. They do a version called the Kairos Blanket Exercise in Canada. And so their exercises focused on First Nations experiences. They came to Alaska a couple of years ago and shared it with us. And the people that participated in that initial one were just so impressed with it that they wanted to bring it to Alaska.
So it is an adaptation of a Canadian exercise. The exercise itself has two parts to it. It has a history lesson and then a talking circle. For the history lesson we have people set up in a circle, a large circle of chairs around blankets. These blankets are spread out across the floor in between all the chairs, and we have participants step onto the blankets and step into the role of Alaska Native people.
When they're stepping onto the blankets, they're stepping onto traditional Alaska Native lands, which is all of Alaska. So at the beginning of the exercise, there are a lot of people on these blankets. There's a lot of blankets spread out all throughout. We also have two narrators who read through the Alaska Native history timeline.
And as they go through the timeline several things happen. The land gets smaller and the number of participants on the land, the number of Alaska Native people also gets smaller. So the things that caused the, the decrease in land or the decrease in people, are all related to actual historical events from the Alaska Native history to represent the loss of both land and people and also the relationship between Alaska Native people and the land.
Anne: And then as people go through the simulation, then what?
Jackie: So the experience itself, the history lesson portion, can be kind of intense. It's very emotional for a lot of people. We also have what we call scrolls and they're quotes from either Alaska Natives or political figures in the state of Alaska.
Some of them are really, really tough. There’s one quote in particular from a man who survived the internment camps.
[00:22:23] Anne: Jackie's talking about the internment camps for the Unangax̂ people during World War II. The US government forced the Unangax̂ to leave the Aleutians in 1942 and live in places like old fish canneries in Southeast Alaska for three years. Conditions were very, very harsh. Back to Jackie.
[00:22:42] Jackie: And he was talking about his baby brother who got double pneumonia and then died and how it was the tiniest coffin he had ever seen. The first time I did the exercise myself, I volunteered to read a quote and that's the one I got. And it was just, it was so hard to make it through and it.
That's only a small, small, small percentage of the amount of pain that family felt, that community felt for that tiny coffin. So it's a very emotional experience. I think it's especially emotional for a lot of Alaska Native participants because even if it's not directly related to an experience they had, or that one that their family might've had, they can relate to it.
There's a lot of things in there that make people think, “Oh, I wonder if that happened in my community.” So it can be quite, quite emotional. We do, I want to mention, highlight a lot of strengths in it. It’s really, truly amazing to see what people focus on. We’ve had peoples say they felt really uplifted at the end.
And that's great. Cause we try to have equal balance. Cause there have been a lot of really great things that have happened. Like Elizabeth Peratrovich, for instance, she's a great example to lift and shine, uplift and shine, or the Alaska Native Brotherhood or the Sobriety Movement. There's a lot of really great things to leave with as well. We don't try to traumatize people and then leave them. We also try to highlight a lot of the strengths and the people who are learning their culture again and who are learning their language and all of the efforts to take people are taking to combat colonization in their own personal lives or in their community.
[00:24:29] Anne: So it's both teaching about the pain so that people understand where Alaska Native communities are coming from and where we as a state are coming from, as well as highlighting that actually there's boundless resilience and boundless strength, and always has been.
[00:24:48] Jackie: Yes, absolutely. That is something that we always try to highlight is the resilience. Despite all of these things that have happened to Alaska Native people, we're still here. And we're still here in great, great numbers, and we're doing a lot of really great things in our communities and in our families. And it's important to highlight those things. It's important not to just always talk about the high rates of this or the high rates of that and this community is struggling with this. There's a lot of really great things happening in Alaska Native communities, too.
Also, another component that we didn't really touch on at all was the talking circle. So that can be another way to get people engaged in conversation. And that's part of every exercise. Our talking circle is open forum and people can talk about whatever they want or they can not talk if they don't want to.
I think that really adds to the experience. We ask that people respect each other's privacy, and not talk about it afterwards. What's talked about in the circle, stays in the circle. From our evaluations, we know that the talking circle at the end has almost as much impact on people as the actual exercise itself.
It's a time for people to kind of provide their own testimony and talk about their own experiences and for people to be vulnerable, if that's what they feel comfortable doing.
[00:26:19] Anne: I could see that being really powerful and scary experience in a lot of ways.
[00:26:27] Jackie: Absolutely.
[00:26:30] Anne: With some of the providers and behavioral health care folks that you work with, how has the Blanket Exercise changed the way they practice or the questions that they might ask to help someone along a healing process?
[00:26:50] Jackie: I think it gives people like a sense of what questions am I not asking? What information do I not have? How can I support people better? And how can I connect with them? We haven't really done any long-term outcome evaluation. That's one of the things we're really interested in doing, because we want to know how people are doing it are how people are incorporating it into their work.
But apart from just what we hear offhand, we don't have any solid answers for that yet.
[00:27:24] Anne: Jackie has big dreams for the Blanket Exercise. She wants to create versions for young people and to bring it to schools. She plans to expand the number of facilitators so that all community organizations, including private companies, can participate in the experience because it can make a difference for people who aren't involved with mental health, too. For example, she said that after managers of a grocery chain with stores in rural Alaska participated, it changed how they interacted with employees and customers. Because of COVID-19, ANTHC is currently working on creating a virtual adaptation of the Blanket Exercise. They'll start offering it for free to everyone in early 2022.
[00:28:08] Anne: What Jackie shared was only a brief piece of Alaska's history and how that history still affects Alaska communities today. It's a lot to sit with. So before we delve even deeper into ways to think about historical trauma and the effects of colonization, I'd like to invite you to take a moment to think about these issues on a more personal level and to ground yourself. If you are in a safe space to do so, maybe close your eyes, take a few deep breaths, and think about where you are and who was on this land before you. You could even consider pausing this podcast and jotting down a few thoughts, feelings, or questions that Jackie's interview brings up for you. Take a moment to reflect and then I'll introduce you to Meda.
[00:29:08] Anne: My next guest is Meda DeWitt, a traditional healer and researcher, who I asked to help me understand historical trauma more broadly and how it shapes communities.
[00:29:19] Meda: [Greeting in Tlingit is not transcribed.] My English name is Meda Witt. My Tlingit names are Tśa Tsée Naakw and Khaat kłaat, adopted Iñupiaq name is Tigigalook, and adopted Northern Cree name is Boss Eagle Spirit Woman. I live Dena’ina lands, that’s Anchorage area. I'm here with my fiancé, Chris Paoli. He and I combined have a total of eight children, seven still at home, and it's beautiful to be here.
[00:30:09] Anne: Meda is also a member of the Mental Health Mosaics Advisory Board. She says Tlingit people have a culture of wellness that stems back at least 20,000 years.
[00:30:21] Meda: So everything is built around best practices that've been tested out and observed over thousands of years. And some people are like, “Oh, 10,000 years.” It's like, no, like 20 plus thousand years. Much, much longer than the anthropologists [say]. Every time they dig something up and they find like, “Oh, we found something 14,000 years old.” my auntie's like, “Well, grandma always said that they just had to dig deeper.”
So our cultural stories are much older and we have a long cultural memory that's a living memory. So they impart these concepts and culture and experience almost in a way that is relatable in a first person. Whereas in the Western systems, it's historical and it's a long time ago. And there's a disconnect.
[00:31:15] Anne: So we need to keep this disconnect in mind when thinking about history.
[00:31:20] Meda: The concept of history is different in the two groups, right? So we're working within a trade barter language, which is English. And English is limited. As you know, it's comprised of multiple different languages and it's heart and soul is based on economic exchange and barter.
So we think that we're speaking about the same language or same words and same concepts, when reality is many times we aren't. So people will be in conversations or they'll have disagreements, and it comes down to the fact that they don't have a shared understanding of what's being said.
So historical trauma is a massive occurrence that happened to a family or a cultural group, a group of people. And in the Western context, it means it happened a long time ago. In more Indigenous and familial structured communities historical trauma is something that has happened to a group of people that has influenced their culture and is a part of who they are.
[00:32:30] Anne: Trauma in one generation can also affect people in future generations by changing the expression of their genes. We are not going to go into the science of epigenetics right now, though you can find links to research on the topic on our website. But Meda and many others say that this idea—that trauma affects us generations down the line—has always been a known truth in many Indigenous cultures. It's called blood memory.
[00:33:00] Meda: We had certain protocols of how to behave, like when you're pregnant. And you don't want to stress the mom out because it affect the behavior of the child after it's born. So knowing that trauma has effect on humans in utero. And we also knew that if there was something that happened in the family line that it could manifest in further generations down.
[00:33:27] Anne: So a quick recap: Historical trauma may have happened generations ago, but we aren't detached from those events and their aftereffects. History reverberates through and shapes life today, it shapes families, and it effects all aspects of health. And it’s not just trauma that passes from generation to generation. It's strength. Meda says we need to think about how we frame the stories we tell.
[00:33:59] Meda: That's like Alaska Natives and American Indians. When we have the capacity to have self-governance and internal sovereignty and sovereignty as a group to make our own choices and to define who we are and how we move through this world—then those stories transition from a painful story of burden into an experience that we share, and then our resilience is our story of strength.
So for instance we have a lot of migration stories. And traditionally with the climate has changed several times, but because of our carbon use and the way that we've been using fossil fuels, it's expedited in how fast it's coming on. But there are other times in our history—we have oral histories. And our oral histories are passed down through story keepers and it has to be done in a very specific way.
And even in inflections of the voice. You have to learn it very specifically to tell these stories and to be considered a traditional story keeper. The Tlingit people used to be interior Canada, and there was melting of the glaciers so they had to go to the coast because the food systems were crashing.
And it was very traumatic. People were dying and they were starving and there was a sickness. And they had to make the choice to leave a space that they loved because they couldn't sustain in those spaces anymore. And so that choice of being able to move, and that process of going through the motions of problem solving and courage and strength and then making it to the coast, that's a part of our traditional resiliency stories—the coming under the glaciers.
Resilience is baked in to the culture. Resilience is baked into these stories and spirit and the way of being connected to the land and to Creator and each other. And those are fundamentally the most important success factors in any group of people that you can have, that connectivity.
[00:36:21] Anne: So where do we go from here? How do we heal from traumas so they don't keep affecting generation after generation? Meda is going to talk a lot more about this in a later episode that specifically focuses on Alaska Native Traditional Healing, a topic that's useful for everyone. But in the meantime, she offers this starting place—acknowledge what happened in the past. She says even this step is going to take time and won't always go smoothly.
Meda: We're going to be wonky and imperfect, like a ragtag band of rebels who made it through several hundreds of years of violence. Right?
And so now it's time to acknowledge what happened and rebuild. And there's definitely people who were privileged and benefited from the colonization. And that's part of this challenge. I challenge people to acknowledge this history and everybody has work to do. So if it's uncomfortable for you to acknowledge what happened and speak about it and feel like it's a responsibility to shift the narrative, then that's where people need to work.
Like step into that space that's uncomfortable and help to elevate this collective narrative. Gosh, you know, like let's just tell the truth.
Anne: It's really, really important to note here that acknowledging the trauma caused by colonization, boarding schools, and other injustices is just one part of the healing process. We also need to acknowledge and change the current systems of oppression that have led to severe inequities in our society, all of which affect everyone's mental health. We're going to discuss that with much more depth in our next episode including during a conversation with Melody Li, a queer therapist of color who is a colony-born migrant from Hong Kong.
[00:38:33] Melody: In the work that I do, I often start with sharing that colonialism, capitalism and white cis-hetero patriarchal hegemony, or domination, are at the root of mental and relational distress. This is very different from what the so-called modern mental health field typically shares. We are taught that mental distress comes from maybe childhood trauma, which is true. From interpersonal conflict, which is true. Or simply arises within the individual on a brain chemistry level, on a neurological level. All of those are true, except it doesn't address the context.
The context in which these distresses are occurring and how colonialism, capitalism, white cis-hetero, patriarchy of course, disproportionately impacts marginalized identities, Black, Indigenous, and People of Color, Two Spirit LGBTQ+ communities, neurodivergent and disabled communities. There are multiple added layers of mental and relational distress when we look at things from a historical, intergenerational and perpetual perspective.
So when we don't intentionally include and bring to light and even focus on how these forces impact our mental and relational wellness then we are perpetuating them within the mental health field. And I think one danger of the practice of the mental health industrial complex is the pathologizing, so diagnosing, and also individualizing these distresses. Saying there's something wrong with this person. Let me put a diagnosis on this person, and offer this person a treatment.
But if these distresses are connected to the systemic and institutional oppressions or violences, then no amount of pathology or individualized treatment is going to help. And that is where we are now.
[00:41:25] Anne: And that is all a lot to take in. This is another good time to ground yourself by taking a few deep breaths, noticing your surroundings, or writing down some reactions or questions. Here's a key takeaway I'd like you to carry into your day: Think about mental health in the context of the larger picture. It's tied to history, land, and systems of oppression. Sometimes we feel alone, but our experiences are connected. Please hold onto those thoughts as we explore these issues more in future episodes.
My thanks go to Meda DeWitt, Cathy Salser, and Erin Willihan for reviewing the episode. Susy Buchanan is editing this project. Aria Phillips wrote our theme music. Dave Waldron is the audio engineer. I'm getting guidance from Jason Lessard at NAMI-Anchorage and from the Mental Health Mosaics Advisory Board -- Cassandra Debaets, Dash Togi, Dana Hilbish, Erica Khan, M.C. MoHagani Magnetek, and Meda DeWitt.
You can find more materials on this subject and other tools for processing your thoughts at mentalhealthmosaics.org. Please rate this podcast to help others find it and share links with everyone you know. I'm Anne Hillman. Thank you for listening.
[00:00:00] Anne: Welcome to Mental Health Mosaics, an exploration of mental health from Out North, which is located on the unceded traditional lands of the Dena'ina People in Anchorage, Alaska. I'm Anne Hillman.
When we talk about mental health we often focus on what's happening to each of us as individuals and how we're dealing with life right now. But humans don't exist in bubbles. What happened in our community's past and what's currently happening, including racism and inequity, affects all of us and our mental health. We can't ignore it. So for the next two episodes we're going to focus on colonization, white supremacist culture, and mental health. Yes -- this is going to be heavy and yes, you are probably going to be uncomfortable.
This episode is kind of a primer -- we'll jump into the basics of how colonization in Alaska is having a long-term impact on mental health, why teaching that history is so important, and have a more philosophical conversation about understanding what historical trauma is.
If you are well-versed in Alaska Native history and understand, especially through personal experience, the effects of intentional cultural destruction, this episode is full of triggers and you may want to skip it. But we don't just talk about trauma, we also talk about strength because every culture and every community has both. If you are a non-Indigenous person, especially one who lives in Alaska, please keep listening. This is just the start of what we all need to know when living on Indigenous lands whether you care about mental health or not. So, without further ado, please meet Jackie, who was willing to provide a pretty intense history lesson.
[00:01:50] Jackie: My name is Jackie Engebretson and my family is from Gulkana, which is in the Copper River region here in Alaska and I'm Ahtna Athabaskan, although I grew up in both Copper Center and Valdez. Currently, I am a senior program manager in the behavioral health department at the Alaska Native Tribal Health Consortium.
[00:02:09] Anne: Well, thank you so much for joining us today. So I'd love to start with conization. What does that mean? And what does that mean in Alaska context?
[00:02:18] Jackie: Colonization would be when an outside country/entity comes into another space and takes over in a sense. They start occupying the land as if it was their own. They start making their own rules and laws as if they were the like supreme leaders of that space. Most often that means they are supplanting local populations. So in the state of Alaska there've been many different colonizing forces. Initially the colonizers would be the Russians, particularly in a Western Alaska and in the Aleutians.
Other areas of Alaska did not have as much of a Russian influence, so they had people like missionaries come in, people like the U. S. army come in, and those were their primary colonizers.
So in those instances, like been particularly areas that were colonized by Russians, you saw Russian orthodoxy takeover. You saw Russian culture, Russian language become more predominant. And then in areas where Christian missionaries came in. You saw Christian churches, Christian schools, and rules centered around Christianity instead of the local indigenous populations.
[00:03:38] Anne: And instead of around local and Indigenous belief systems?
[00:03:40] Jackie: Correct, yes.
[00:03:42] Anne: Why is that damaging?
[00:03:45] Jackie: So you have a group of people in the state of Alaska, that'd be Alaska Nativesm who have occupied the land for tens of thousands of years. And they have used the land in ways that feed their family, that nourish their soul, and it's their home.
And all of a sudden you have these people coming in who have a different viewpoint when it comes to how you use land. With Russians, they did a lot of trapping and hunting and over trapped and over hunted resources that Alaska Native people have been using for many, many years without impacting the animal populations.
Resources that were once available are no longer available. You have people occupying spaces that were historically yours. That could be places where your family used to gather food. That could be places where your family used to go to practice spiritual practices. That could be places where your family has just traditionally occupied and all of a sudden there are Russians or Americans living in this land and telling you that you can no longer use it. And it can impact the way you hunt and just it impacts all ranges of your life.
[00:05:03] Anne: And does it impact mental health?
[00:05:05] Jackie: Yes, it can absolutely impact mental health. That's some of the things that we see more long-term here in Alaska.
Particularly as colonization continues. There's like restrictions on how you can hunt, when you can hunt, who else is allowed to hunt, and who else is on your land. They're telling you what you must believe. When your whole way of life is just shifted that way, you lose many different protective factors. And so protective factors are things that kind of keep you mentally and physically safe. So with Alaska Native people -- with people in general, to be honest, this is not just a Native thing -- but identity is a huge part of what helps people feel more rooted in who they are.
And in the United States, there is a general lack of identity, not just with Alaska Native people, not just with Indigenous people. There are a large number of people in this country who just don't have that sense of identity that maybe previous generations would have or maybe other groups throughout the world do have.
[00:06:11] Anne: Just because in the United States, there's is this giant push towards assimilation, and we are all the same, and there is a dominant culture and, and it sort of eliminates our roots and our connections.
[00:06:23] Jackie: Absolutely. And so that's especially true here in Alaska with Alaska Native people. The long-term impacts of colonization might include things like I mentioned, not being able to hunt. So for a lot of Alaska Native men, for instance they had roles that they were expected to fulfill including hunting and gathering and things like that. And now those roles are limited and they no longer have the same ability to do things that they might have previously.
Historically, my people were semi-nomadic so they would move from camp to camp depending on the season. They'd have fish camp and they'd have a hunting camp and they'd have places they'd go to pick berries and things like that. And that was down to the family level.
But after colonization, there was a huge push for families to stay in one spot so that the kids could go to school. “This is in the best interest of your kids. And if you want them to have a good education and a good life, then you need to stay here in this village and your kids need to go to school. They need to go to school following this schedule and that schedule doesn't follow subsistence hunting.
It doesn't follow it -- doesn't follow anything. It follows this arbitrary date that the U.S. government or the state government has told kids that they must be in school. So things like that. You're not following your own traditional and cultural practice. Instead, you're doing what is expected of you by the U.S. government.
[00:07:52] Anne: And at the same time, there's still a practical need to hunt and gather in rural Alaska to get the food and nutrition people need to survive.
[00:08:02] Jackie: We know what naturally grows in Alaska and how we receive our nutrients. You know, traditional Alaska Native diets fulfilled all the nutritional needs. And without eating all of those foods, you're not getting the same needs and instead you need to supplement them with things that you might get from the grocery store. And the items that you might get to supplement your nutritional needs from the grocery store might be extremely expensive because it needs to be shipped up from the United States.
You might have to take vitamins and things like that. So I think from a practical purpose, it's something that's still necessary today. There’s a nutritional basis. And then just the spiritual connectedness that comes from hunting and gathering and being connected to the land and being part of and having a relationship with the land that you have for tens of thousands of years is also still important.
[00:08:56] Anne: And that, again, brings us back to mental health and how these spiritual connections keep us well. I mean, physically well, but also well as whole people. You mentioned earlier, it's not just restrictions on land. Just limiting of land use and movement that happened through colonization, but you also mentioned that churches and missionaries came in.
How did that affect the Indigenous peoples of Alaska?
[00:09:30] Jackie: Yeah, I think the most notable example and one that's probably most relevant to the discussion today would be boarding schools. So throughout the state there were -- and this is honestly something that's an international thing is not something that just happened here in Alaska. We've seen a lot of talk about it in the news recently, due to mass graves being uncovered in Canada. Mass unmarked graves from children in Canada, children that were never returned home.
So the boarding schools were set up to assimilate Indigenous youth. And there was this mentality at the time where the idea was to “save the man and kill the Indian.”
So you save the man by sending them to school, to this boarding school, away from their family, away from their community. And you kill the Indian by not allowing them to speak their language, by not allowing them to be raised by their community and not practice their spiritual practices, their traditional practices, not allowing them to sing their songs, not allowing them to dance.
And by the time you're done with them with them, by the time they were done with boarding school, if they survived, they would be sent back to their communities and no longer feel a sense of identity. Or feel very disconnected from their identity. Not only from their identity, but from their family, from their mom, their dad, from their community.
And many people who go into boarding school just never returned to their community, whether it be because they passed away or because they just no longer felt like they were a part of their community. One of the ways that they would assimilate was by not allowing them to speak their language and children would be punished.
I've heard many stories from elders and I think a lot of other people have heard other stories as well. Punishment, like restricting food, not allowing them to eat. Physical punishment, whether it be spanking, beating, a lot of really terrible, terrible things happened to children in boarding schools.
[00:11:33] Anne: And just a side note here -- the boarding schools in Alaska were started by missionaries. By the early 20th century, they were run by the federal government. It was the U.S. government's policy to take children away from their families and sometimes send them to the other side of the continent. And all of this led to really negative long-term consequences that we still feel today. This isn't just a history lesson. Boarding schools have created persistent, intergenerational trauma. Back to Jackie.
[00:12:06] Jackie: Because they weren't raised by their families, a lot of youth who went through boarding schools didn't have a model of what parenting should look like. So when they grew up to be adults, they had hard time parenting themselves.
They might not have been the healthiest parents. They might not have been the most present parents. It had a lot of long-term impacts on parenting. It had a lot of long-term impacts on people's mental health and their physical health. We know that when people experience Adverse Childhood Experiences that there's long-term impacts to that. It could affect your physical health. It's higher rates of diabetes, higher rates of obesity. It can impact their mental health. They're more likely to interact with the criminal justice system. All of those, I mean like many more things as well.
[00:12:56] Anne: Use substances?
[00:12:57] Jackie: Use substances. Exactly. Exactly. Substance use rates are also very, very high for people who have high ACE scores. Going to a boarding school is just a number of ACEs that add on, with an added aspect of like racism in it as well.
[00:13:16] Anne: Talk more about the aspect of racism. I mean the obvious eliminate who you are and eliminate cultures.
[00:13:24] Jackie: Yeah. So all of this was rooted in the idea, like I mentioned of kill the Indian, save the man. So the idea is that since colonization here in the United States and worldwide as well, is that people of non-European descent are lesser than. They're like lesser than human often, but they're certainly lesser than their white counterparts. So there was this idea that American Indians and Alaska Natives and other populations worldwide were savage or that they were uncivilized or that they were backwards.
And just this idea that they were not equal and that they needed to change. And that colonization was to save them and was a good thing for them. And that European people were supreme and were just more civilized and therefore were doing you a favor. So there was a racial component in the boarding schools because they wanted Native youth to be more like white people.
[00:14:31] Anne: Thinking about this intentional move to cut people off from their families, to cut people off from their culture, to try to make them into someone else. I feel like that hasn't stopped to this day, so how does that relate to behavioral health? Like why do you as a behavioral health organization work to make sure that people understand the complexities of these issues?
[00:15:02] Jackie: That's a great question. I can use myself as an example if that helps.
The reason why this kind of work is really important to me is because of my own kind of lived experiences and things that I've seen in my family, friends, my community. But talking about me specifically since it's my story and my place to tell. I grew up in a very complicated family system. And I know that we all loved each other, but there was trauma that was carried over through generations.
My parents experienced trauma from their parents and my grandparents experienced trauma from their parents. I honestly don't know how far back it goes, but I would imagine it goes back pretty far.
And I think some of it is rooted in some of the things that happen to our community and perhaps how people were treated many, many generations ago that still shows up today. And so I grew up thinking that there was something wrong with me, thinking that there was something wrong with my family and that there was something wrong with my community. Some of the challenges that I had in my own life -- I struggled with depression. I still do. And then eventually I struggled with substance use, and I thought that was because I was Native. And I thought it was because there was something wrong with my family. And I thought that it was just kind of my destiny and like it was going to happen. And it was inevitable.
[00:16:28] Anne: Just because you were Native?
[00:16:30] Jackie: Yeah, because the messages I received, I think from everybody. Everybody gave you these messages. Um, certainly when I was in school, I was a high achiever. I didn't have a lot of Native friends when I was in high school. And I would hear people say things about Natives and I'd be like, “Oh, they're not talking about me though.”
It like took until I had become an adult to really understand. It's like, well, even if they weren't talking about me, they were definitely talking about some of my cousins. Or they're definitely talking about my auntie or my uncle. So yes, they were talking about me, and I just thought I was like one of the good ones when I was in high school or something. And then I had this like crashing reality when I was on my own and an adult and trying to just deal with all these complicated things that I had experienced in life and wondering what's wrong with me. And I know that this is true for other people all over the place.
And I know that there are still people who are living in these really complicated patterns in their life because of historical trauma, because of intergenerational trauma. Who are internalizing that and thinking that there's something wrong with them or maybe thinking that there's something wrong with everybody around them. And not understanding that there's been a lot of things that have happened to us as a people, as family systems that are just really difficult to overcome. And unless you have access to resources and unless you're aware of what's going on, you're not going to be able to get the help. You're not going to, or you might not even want to. And if you think that there's something wrong with you, you're going to think there's probably something wrong with going to therapy or there's probably something wrong with going to treatment. Or there's something wrong with taking medications that can help manage your mental health.
So there's like all these really complex thought processes that go on with people. And the added like racism and stigma associated with a lot of the things we talked about, substance use, mental health, being involved in the criminal justice system, that just like all these different barriers that make people not want to access care.
So the reason why we at ANTHC decided to share the Alaska Blanket Exercise widely is because we wanted providers to understand, “Hey, your patient, isn't just not showing up or like not taking their medication because they don't want to, or because they're willfully being ignorant they're willfully being bad patients. It's because they have a lot of things going on in their lives and they're doing the best that they can to show up. And you need to understand this. You need to understand their traumas.”
It's to help Alaska Native people understand, "Hey, this is, this might be why your family is the way that they are, and there's nothing wrong with you. It's just, there's, there's been a lot that has happened." It think it just helps people be more compassionate for others and for themselves.
[00:19:33] Anne: Explain what this Blanket Exercise is.
[00:19:40] Jackie: Sure. So the Alaska Blanket Exercise is a participatory history lesson. We initially partnered with a Canadian organization called Kairos. They do a version called the Kairos Blanket Exercise in Canada. And so their exercises focused on First Nations experiences. They came to Alaska a couple of years ago and shared it with us. And the people that participated in that initial one were just so impressed with it that they wanted to bring it to Alaska.
So it is an adaptation of a Canadian exercise. The exercise itself has two parts to it. It has a history lesson and then a talking circle. For the history lesson we have people set up in a circle, a large circle of chairs around blankets. These blankets are spread out across the floor in between all the chairs, and we have participants step onto the blankets and step into the role of Alaska Native people.
When they're stepping onto the blankets, they're stepping onto traditional Alaska Native lands, which is all of Alaska. So at the beginning of the exercise, there are a lot of people on these blankets. There's a lot of blankets spread out all throughout. We also have two narrators who read through the Alaska Native history timeline.
And as they go through the timeline several things happen. The land gets smaller and the number of participants on the land, the number of Alaska Native people also gets smaller. So the things that caused the, the decrease in land or the decrease in people, are all related to actual historical events from the Alaska Native history to represent the loss of both land and people and also the relationship between Alaska Native people and the land.
Anne: And then as people go through the simulation, then what?
Jackie: So the experience itself, the history lesson portion, can be kind of intense. It's very emotional for a lot of people. We also have what we call scrolls and they're quotes from either Alaska Natives or political figures in the state of Alaska.
Some of them are really, really tough. There’s one quote in particular from a man who survived the internment camps.
[00:22:23] Anne: Jackie's talking about the internment camps for the Unangax̂ people during World War II. The US government forced the Unangax̂ to leave the Aleutians in 1942 and live in places like old fish canneries in Southeast Alaska for three years. Conditions were very, very harsh. Back to Jackie.
[00:22:42] Jackie: And he was talking about his baby brother who got double pneumonia and then died and how it was the tiniest coffin he had ever seen. The first time I did the exercise myself, I volunteered to read a quote and that's the one I got. And it was just, it was so hard to make it through and it.
That's only a small, small, small percentage of the amount of pain that family felt, that community felt for that tiny coffin. So it's a very emotional experience. I think it's especially emotional for a lot of Alaska Native participants because even if it's not directly related to an experience they had, or that one that their family might've had, they can relate to it.
There's a lot of things in there that make people think, “Oh, I wonder if that happened in my community.” So it can be quite, quite emotional. We do, I want to mention, highlight a lot of strengths in it. It’s really, truly amazing to see what people focus on. We’ve had peoples say they felt really uplifted at the end.
And that's great. Cause we try to have equal balance. Cause there have been a lot of really great things that have happened. Like Elizabeth Peratrovich, for instance, she's a great example to lift and shine, uplift and shine, or the Alaska Native Brotherhood or the Sobriety Movement. There's a lot of really great things to leave with as well. We don't try to traumatize people and then leave them. We also try to highlight a lot of the strengths and the people who are learning their culture again and who are learning their language and all of the efforts to take people are taking to combat colonization in their own personal lives or in their community.
[00:24:29] Anne: So it's both teaching about the pain so that people understand where Alaska Native communities are coming from and where we as a state are coming from, as well as highlighting that actually there's boundless resilience and boundless strength, and always has been.
[00:24:48] Jackie: Yes, absolutely. That is something that we always try to highlight is the resilience. Despite all of these things that have happened to Alaska Native people, we're still here. And we're still here in great, great numbers, and we're doing a lot of really great things in our communities and in our families. And it's important to highlight those things. It's important not to just always talk about the high rates of this or the high rates of that and this community is struggling with this. There's a lot of really great things happening in Alaska Native communities, too.
Also, another component that we didn't really touch on at all was the talking circle. So that can be another way to get people engaged in conversation. And that's part of every exercise. Our talking circle is open forum and people can talk about whatever they want or they can not talk if they don't want to.
I think that really adds to the experience. We ask that people respect each other's privacy, and not talk about it afterwards. What's talked about in the circle, stays in the circle. From our evaluations, we know that the talking circle at the end has almost as much impact on people as the actual exercise itself.
It's a time for people to kind of provide their own testimony and talk about their own experiences and for people to be vulnerable, if that's what they feel comfortable doing.
[00:26:19] Anne: I could see that being really powerful and scary experience in a lot of ways.
[00:26:27] Jackie: Absolutely.
[00:26:30] Anne: With some of the providers and behavioral health care folks that you work with, how has the Blanket Exercise changed the way they practice or the questions that they might ask to help someone along a healing process?
[00:26:50] Jackie: I think it gives people like a sense of what questions am I not asking? What information do I not have? How can I support people better? And how can I connect with them? We haven't really done any long-term outcome evaluation. That's one of the things we're really interested in doing, because we want to know how people are doing it are how people are incorporating it into their work.
But apart from just what we hear offhand, we don't have any solid answers for that yet.
[00:27:24] Anne: Jackie has big dreams for the Blanket Exercise. She wants to create versions for young people and to bring it to schools. She plans to expand the number of facilitators so that all community organizations, including private companies, can participate in the experience because it can make a difference for people who aren't involved with mental health, too. For example, she said that after managers of a grocery chain with stores in rural Alaska participated, it changed how they interacted with employees and customers. Because of COVID-19, ANTHC is currently working on creating a virtual adaptation of the Blanket Exercise. They'll start offering it for free to everyone in early 2022.
[00:28:08] Anne: What Jackie shared was only a brief piece of Alaska's history and how that history still affects Alaska communities today. It's a lot to sit with. So before we delve even deeper into ways to think about historical trauma and the effects of colonization, I'd like to invite you to take a moment to think about these issues on a more personal level and to ground yourself. If you are in a safe space to do so, maybe close your eyes, take a few deep breaths, and think about where you are and who was on this land before you. You could even consider pausing this podcast and jotting down a few thoughts, feelings, or questions that Jackie's interview brings up for you. Take a moment to reflect and then I'll introduce you to Meda.
[00:29:08] Anne: My next guest is Meda DeWitt, a traditional healer and researcher, who I asked to help me understand historical trauma more broadly and how it shapes communities.
[00:29:19] Meda: [Greeting in Tlingit is not transcribed.] My English name is Meda Witt. My Tlingit names are Tśa Tsée Naakw and Khaat kłaat, adopted Iñupiaq name is Tigigalook, and adopted Northern Cree name is Boss Eagle Spirit Woman. I live Dena’ina lands, that’s Anchorage area. I'm here with my fiancé, Chris Paoli. He and I combined have a total of eight children, seven still at home, and it's beautiful to be here.
[00:30:09] Anne: Meda is also a member of the Mental Health Mosaics Advisory Board. She says Tlingit people have a culture of wellness that stems back at least 20,000 years.
[00:30:21] Meda: So everything is built around best practices that've been tested out and observed over thousands of years. And some people are like, “Oh, 10,000 years.” It's like, no, like 20 plus thousand years. Much, much longer than the anthropologists [say]. Every time they dig something up and they find like, “Oh, we found something 14,000 years old.” my auntie's like, “Well, grandma always said that they just had to dig deeper.”
So our cultural stories are much older and we have a long cultural memory that's a living memory. So they impart these concepts and culture and experience almost in a way that is relatable in a first person. Whereas in the Western systems, it's historical and it's a long time ago. And there's a disconnect.
[00:31:15] Anne: So we need to keep this disconnect in mind when thinking about history.
[00:31:20] Meda: The concept of history is different in the two groups, right? So we're working within a trade barter language, which is English. And English is limited. As you know, it's comprised of multiple different languages and it's heart and soul is based on economic exchange and barter.
So we think that we're speaking about the same language or same words and same concepts, when reality is many times we aren't. So people will be in conversations or they'll have disagreements, and it comes down to the fact that they don't have a shared understanding of what's being said.
So historical trauma is a massive occurrence that happened to a family or a cultural group, a group of people. And in the Western context, it means it happened a long time ago. In more Indigenous and familial structured communities historical trauma is something that has happened to a group of people that has influenced their culture and is a part of who they are.
[00:32:30] Anne: Trauma in one generation can also affect people in future generations by changing the expression of their genes. We are not going to go into the science of epigenetics right now, though you can find links to research on the topic on our website. But Meda and many others say that this idea—that trauma affects us generations down the line—has always been a known truth in many Indigenous cultures. It's called blood memory.
[00:33:00] Meda: We had certain protocols of how to behave, like when you're pregnant. And you don't want to stress the mom out because it affect the behavior of the child after it's born. So knowing that trauma has effect on humans in utero. And we also knew that if there was something that happened in the family line that it could manifest in further generations down.
[00:33:27] Anne: So a quick recap: Historical trauma may have happened generations ago, but we aren't detached from those events and their aftereffects. History reverberates through and shapes life today, it shapes families, and it effects all aspects of health. And it’s not just trauma that passes from generation to generation. It's strength. Meda says we need to think about how we frame the stories we tell.
[00:33:59] Meda: That's like Alaska Natives and American Indians. When we have the capacity to have self-governance and internal sovereignty and sovereignty as a group to make our own choices and to define who we are and how we move through this world—then those stories transition from a painful story of burden into an experience that we share, and then our resilience is our story of strength.
So for instance we have a lot of migration stories. And traditionally with the climate has changed several times, but because of our carbon use and the way that we've been using fossil fuels, it's expedited in how fast it's coming on. But there are other times in our history—we have oral histories. And our oral histories are passed down through story keepers and it has to be done in a very specific way.
And even in inflections of the voice. You have to learn it very specifically to tell these stories and to be considered a traditional story keeper. The Tlingit people used to be interior Canada, and there was melting of the glaciers so they had to go to the coast because the food systems were crashing.
And it was very traumatic. People were dying and they were starving and there was a sickness. And they had to make the choice to leave a space that they loved because they couldn't sustain in those spaces anymore. And so that choice of being able to move, and that process of going through the motions of problem solving and courage and strength and then making it to the coast, that's a part of our traditional resiliency stories—the coming under the glaciers.
Resilience is baked in to the culture. Resilience is baked into these stories and spirit and the way of being connected to the land and to Creator and each other. And those are fundamentally the most important success factors in any group of people that you can have, that connectivity.
[00:36:21] Anne: So where do we go from here? How do we heal from traumas so they don't keep affecting generation after generation? Meda is going to talk a lot more about this in a later episode that specifically focuses on Alaska Native Traditional Healing, a topic that's useful for everyone. But in the meantime, she offers this starting place—acknowledge what happened in the past. She says even this step is going to take time and won't always go smoothly.
Meda: We're going to be wonky and imperfect, like a ragtag band of rebels who made it through several hundreds of years of violence. Right?
And so now it's time to acknowledge what happened and rebuild. And there's definitely people who were privileged and benefited from the colonization. And that's part of this challenge. I challenge people to acknowledge this history and everybody has work to do. So if it's uncomfortable for you to acknowledge what happened and speak about it and feel like it's a responsibility to shift the narrative, then that's where people need to work.
Like step into that space that's uncomfortable and help to elevate this collective narrative. Gosh, you know, like let's just tell the truth.
Anne: It's really, really important to note here that acknowledging the trauma caused by colonization, boarding schools, and other injustices is just one part of the healing process. We also need to acknowledge and change the current systems of oppression that have led to severe inequities in our society, all of which affect everyone's mental health. We're going to discuss that with much more depth in our next episode including during a conversation with Melody Li, a queer therapist of color who is a colony-born migrant from Hong Kong.
[00:38:33] Melody: In the work that I do, I often start with sharing that colonialism, capitalism and white cis-hetero patriarchal hegemony, or domination, are at the root of mental and relational distress. This is very different from what the so-called modern mental health field typically shares. We are taught that mental distress comes from maybe childhood trauma, which is true. From interpersonal conflict, which is true. Or simply arises within the individual on a brain chemistry level, on a neurological level. All of those are true, except it doesn't address the context.
The context in which these distresses are occurring and how colonialism, capitalism, white cis-hetero, patriarchy of course, disproportionately impacts marginalized identities, Black, Indigenous, and People of Color, Two Spirit LGBTQ+ communities, neurodivergent and disabled communities. There are multiple added layers of mental and relational distress when we look at things from a historical, intergenerational and perpetual perspective.
So when we don't intentionally include and bring to light and even focus on how these forces impact our mental and relational wellness then we are perpetuating them within the mental health field. And I think one danger of the practice of the mental health industrial complex is the pathologizing, so diagnosing, and also individualizing these distresses. Saying there's something wrong with this person. Let me put a diagnosis on this person, and offer this person a treatment.
But if these distresses are connected to the systemic and institutional oppressions or violences, then no amount of pathology or individualized treatment is going to help. And that is where we are now.
[00:41:25] Anne: And that is all a lot to take in. This is another good time to ground yourself by taking a few deep breaths, noticing your surroundings, or writing down some reactions or questions. Here's a key takeaway I'd like you to carry into your day: Think about mental health in the context of the larger picture. It's tied to history, land, and systems of oppression. Sometimes we feel alone, but our experiences are connected. Please hold onto those thoughts as we explore these issues more in future episodes.
My thanks go to Meda DeWitt, Cathy Salser, and Erin Willihan for reviewing the episode. Susy Buchanan is editing this project. Aria Phillips wrote our theme music. Dave Waldron is the audio engineer. I'm getting guidance from Jason Lessard at NAMI-Anchorage and from the Mental Health Mosaics Advisory Board -- Cassandra Debaets, Dash Togi, Dana Hilbish, Erica Khan, M.C. MoHagani Magnetek, and Meda DeWitt.
You can find more materials on this subject and other tools for processing your thoughts at mentalhealthmosaics.org. Please rate this podcast to help others find it and share links with everyone you know. I'm Anne Hillman. Thank you for listening.
Ways to Decolonize
Ways to decolonize mental health
[00:00:00] Anne: Welcome to Mental Health Mosaics, an exploration of mental health from Out North, which is located on the unceded traditional lands of the Dena'ina People in Anchorage, Alaska. I'm Anne Hillman.
On the last episode of Mental Health Mosaics we spoke about colonization, historical trauma, the intentional and ongoing destruction of Indigenous culture and identity, and how all of that relates to mental health. Yeah, it was a lot, and it was really only a fraction of all of the community-wide things we need to consider when talking about mental health.
And though we talked about the traumas that have long-term effects on communities, we also talked about the strengths and we touched very, very briefly on healing. -- Thanks, Meda! -- Never fear -- every episode of Mental Health Mosaics will also highlight ways to heal or move forward. Maybe that's in part because I'm annoyingly an eternal optimist and I'm the producer of this show, but mostly it's because there really are people who are striving to make the world better -- meaning more equitable -- for everyone.
In this episode I want to introduce you to two of those people. First is Melody Li.
[00:01:17] Melody: Hi everyone. My name is Melody Li and I use pronouns car in Cantonese and any in English. And I am a colony-born migrant, and a diasporic settler here on Turtle Island. I am a queer therapist of color. And also a mental health, um, liberation activist through our work in community at Inclusive Therapists.
[00:01:49] Anne: Melody is from Hong Kong and currently lives in Austin, Texas. I came across her work when I was trying to understand how mental health treatment is shaped by white supremacy culture. I know that some of you just flinched when I said those words. It's still something I'm getting used to saying in this context as well, and it’s a term that’s hotly debated. Is it useful? Divisive? Definitely a point of debate. Melody doesn’t actually use it in this conversation. She uses Eurocentric domination.
When I say white supremacy, I'm not talking about hate groups. Right now I’m not even talking about structural racism -- we’ll get to that in other episodes. I'm talking about how white ideas of what is right dominate our culture. These ideas are well laid out by Tem-uh O-kun in a whole website on white supremacy culture.
Think about the values that we often don’t even question, like individualism, perfectionism, and objectivity. This culture is why we primarily value knowledge when it comes with a degree or a published work, usually from a white-led institution. Many of us define success by gaining power and resources -- progress means getting bigger. White supremacist culture also defines professionalism by white standards and falls back on white-determined qualifications when promoting people in organizations. And it simplifies issues into either/or binaries -- you’re good or bad, that’s right or wrong. It doesn’t allow for nuances.
These ideas reign supreme and we all have them ingrained in us whether we want them to be or not. They originate in the creation of the United States which said white people should dominate all others, and they permeate well beyond our borders. There are links to many articles discussing these ideas on the Mental Health Mosaics website. Please check them out -- my explanation is limited because I’m still learning and I definitely welcome feedback. And I give many thanks to the folks at Native Movement who offer training that helped me start to notice this culture in ways I hadn’t before.
But back to Melody -- I sought them out because I wanted to learn from someone who is actively examining how white ideals shape what mental health treatment looks like and is advocating for change. They want to decolonize mental health, which means looking both at what happens in a therapy session and beyond. This is Melody:
[00:02:57] Melody: So we as a mental health field, um, dominate -- have a Eurocentric domination of what we consider to be valid. What we consider to be true knowledge or valid knowledge. And we gatekeep that through institutions of school, of our trainings of who gets to be licensed, who doesn't and which often not only neglects, but attempts to erase the lived experiences of Black Indigenous and people of color. And so it's a very limited knowledge base, but we try to pretend that these, this knowledge is universal because of colonial ideology.
Um, Another way that, um, coloniality shows up through the mental health field is the monopolizing of power through Eurocentric or American centric ontology, or how do we conceptualize what is reality? What is beinghood? What is personhood? What is humanity?
Anne: So I think I need a little bit more on that. Like... absolutely um, so one thing that we see often is, um, again for marginalized communities that may believe that one's being-hood is an interconnection with land, with non-humans, with animals, with plants, with water. These are our relatives. These are Indigenous practices here on Turtle Island, but also Indigenous, um, practices, um, across the globe.
And that our beinghood is also in interconnection with the spiritual, with the cosmos. Um, but, but when that is deemed um, not true through Eurocentric ontology, then we become quickly pathologized again. "Oh, this person, um, is dissociating." "This person doesn't have self-esteem or self-concept."
[00:05:11] Anne: Okay.
[00:05:12] Melody: Or when our reality is also, um, being questioned, um, there are folks that for example, may see visions or may hear, um, voices in interconnection with other beings. And when we are limited by Eurocentric ontology, then again, we pathologize and say, this person is. Um, we say all types of horrible, stigmatizing things, as opposed to saying, wow, there are actually different realities and different ways of being, and that is also a way that Eurocentric, um, psychology is very harmful.
[00:05:52] Anne: And so, seeing things just through a medicalized, Westernized system says things are wrong when really they're just not how other people experience life.
[00:06:04] Melody: Yes. Not how we experience and understand life. And so when I hear about stigma towards mental illness, how this is often used as blame on marginalized communities, especially, you know, Black, Indigenous, POC communities. We’re often blamed for not seeking mental health care. And we're often blamed to say, well, we, the people of color, stigmatize mental health and therapy, that's why they don't pursue it.
I always push back and I ask who stigmatized whom. That if we know that our ways of being and our realities and our understanding of personhood is not going to be honored and will be pathologized, that is a very risky situation to enter into.
And I can list so many examples. I come from a relatively collectivist culture, but when there's a Eurocentric lens that's put on our family models, our family systems, for example, we're often told that we are enmeshed. There's too much enmeshment. T here needs to be more individualism, um, self, self-concept, right? And this is actually really common and we're trained to look at what is wrong as opposed to valuing our ways of being. And this conceptualization is also very much interconnected with all the, what we call so-called phobias and isms, you know, gender binary, heteronormativity, um, fatphobia, classism, ableism. Christian centrism and all of this is embedded in the mental health field and we, we need to have a really honest and brave look at the ways that we are upholding this and are perpetuating harm through what we are selling as treatment or healing.
[00:08:31] Anne: You have used terms like decolonizing mental health. What does that mean?
[00:08:39] Melody: So Bhatia shares: it is about reclaiming water, land, territory, and language.
Decolonization means restoring what was lost.
That's where we start, because it's the water, land, language, culture, our ways of being that we're, that we're severed from that is the root of mental distress. So we're not starting with the symptoms. It's looking at what was lost and what is our role in the restoration. Um, restoration there is reparation.
Um, and, and for, for folks that have experienced colonization, this process is different from people that have inherited privilege through colonialism. Um, so for example, you know, in addition to land back, water back, that is always at the root, for, for simplicity’s sake, I'm going to say BIPOC or folks of color, for us it's all also about reclaiming our, our ways of being in our healing practices.
For folks that for example, may be descendants of colonial settlers, white colonial settlers, their work looks different. It means returning. Giving back. It means reparations. It means reorganizing, so now that we know that these hegemonic, you know, dominant, systemic, structures are in place. Those need to be dismantled.
And so there's, there are multiple processes, um, that happen simultaneously. Um, but if I were to simplify it, I would say, let's start with, um, focusing on, and this I'm learning from Indigenous communities, land back, Indigenous sovereignty and Black liberation. If the work that we do is not grounded in that, then there, we are always at risk of practicing in an exploitative manner, like something that is exploitive to communities of colors and Indigenous communities.
Um, and, and so in terms of the, how -- we got to do it in community. Because it's not something that can again be individualized. It's not a person saying, okay, I'm going to restructure my therapy practice and I'm going to read books because colonialism and coloniality. It's unfortunately embodied and also integrated in our mindsets.
And there, oftentimes we may not be aware of the ways that we can be oppressive, that we can be violent. And so being in community means that we, um, learn from one another, but also we, um, have systems of accountability that we talk about what rupture and repair means, that we look around corners from one another. We correct one another. And so I believe that decolonizing mental health care has to happen in community. And it's also a relational process between humans, but certainly. Non-humans and more than humans as well.
[00:12:31] Anne: And so and please, correct me if I'm wrong. I hear what you're saying in what you're saying, but it's not like we can just say, okay, let's do X, Y, or Z to mental health. To fix the mental healthcare system, we have to do it in concert with fixing all of these others systems. And that we need to do it while listening and making amends and accepting that that's going to look really different for everybody.
[00:13:02] Melody: Yes. It's going to look different depending on, gonna use that word, positionality, which means that we are made up of different social identities.
And some of our social identities hold more power. Some of our social identities may be marginalized and each of us have a unique combination or makeup of that. But when we look at our positionality, for example, some of my parts are, um, I have. Uh, skin color privilege. Um, I have non-disabled privilege. I have education and class background privilege.
However, there are other parts of me as I shared, um, my queerness, um, being a colony born person, being an immigrant. These are parts that are marginalized. I have to bring -- I'm bringing all of these parts in the work that I do in community. I bring all these parts also in the therapeutic setting. So I need to be mindful of not only my positionality, how I show up in relationships with others, but also in relations to this land. My position on this land is yes, I'm a diasporadic settler, but I'm a settler. This is not my land, so what is my responsibility as I'm on this land as a visitor, as a migrant, as a person seeking refuge?
That is different from someone with a different set of social identities that have a different relationship with this land. And, um, so, so that's why it's not really, um, possible to have an ABC because it requires us to bring our full beings in here, and these interactions are relational. At the same time, there are practical things we can do such as, um, learning, learning from Indigenous communities and writers and activists following their lead, following the lead of Black activists.
Um, and there's so much learning that we can do. And also I think an important part is healing. That if we're injured, if we have, um, injured through racialized trauma, or we have been, um, yeah, that even for white folks, when white folks were not always white folks. White folks belong somewhere, but when they are either displaced, um, or when they had to, um, not have to some chose to move away from their place of origin and give up their cultural identities, um, to trade in for power that, that there are ruptures there that happen as well. And that require healing because if we don't also, as practitioners focus on our healing, then we are more at risk of perpetuating, hurt, and harm and injuries on to others.
[00:16:27] Anne: So in this world where you're balancing these two things like your livelihood and seeing individual patients, as well as creating new structures, how do you bring this greater systemic work and this greater dismantling work into that individual practice? Like how are you trying to transition this Western model of sitting down one-on-one and talking to people into something that really is more inclusive and also more acknowledging just the reality of, of our intersectional identities in of our positionality.
[00:17:10] Melody: Um, the first thing that came to mind, I love this question is. I'm realizing that this is not on me, that my offerings are, are just, limited to what I, as one person can offer. So part of my work is to learn about, to connect with folks with different, um, ways of healing, different wellness practices, and being well resourced so that when a service user, you know, meets with me, I understand my limitations.
And this is something that we, as a field are, is not good at. That we, because in order to maintain power, we sell this image that we know at all, that we have all the answers, but actually what we need to know is our limitations. That my limitations are limited to my lived experiences, to my ancestral practices that may or may not be helpful for somebody else.
However, um, there are, I, I can hold space for someone I can, um, guide them to also look at their intergenerational lineage traumas. I can hold space for conversation about how oppression and a racialized violence impact them and their psyche and their relationships. So I can hold space for a lot of these relationships, these conversations, those dialogue, but I also need to be aware of different healing modalities that exist that can be helpful for them.
So that is one way. Another way is that, um, also creating these new systems of collective care that is not necessarily dependent on systems like insurance panels or, um, you know, capitalistic systems that are community funded. So that's something that our communities work really hard on. How do we extend care in a way um, honors the service users. And, um, and their needs, especially financial needs, but it's also, um, it's also sustaining to healers and therapists. So the work that I do, um, in the therapy room per se, it looks different during COVID is yes, we absolutely have one-on-one time. There is space for one-on-one time, but I am mindful that this, this 50 minutes I'm spending with this person once a week or every other week is only a slice of the possibilities of healing.
And can I offer them more? Um, and at the same time, am I also advocating for them outside of the therapy room?
[00:20:34] Anne: And it really highlights something that I feel like people are more and more realizing. Most people I've been speaking with are more and more realizing that like therapy in these conventional group therapy, individual therapy, these conventional ways that we've all been taught to seek help aren't the only ways. And seeking help by being part of a community garden, seeking help by just listening to people, seeking help through, you know, offering, offering food at a community fridge are always to also heal and be part of things.
[00:21:15] Melody: Yes, those are really the ways that, um, that get me excited that, um, because this mutual aid, um, is restorative to entire communities, not just the folks that are hurting. It's for all of us.
And so, so much more to this, and also reminding us that Mother Earth is so good to us, that there's so much healing that exists, that, you know, they so lovingly and generously offer us. But that we are not good stewards of,That through capitalism, we have disconnected from our, even are destroying. So part of our healing is also asking how do we return to a relationship, a respectful, loving, reciprocal relationship with Mother Earth. If the land is not well, if the water is not well, how can we possibly be mentally well?
[00:22:35] Anne: you say like we have this duty to the land around us, to the water around us. What sort of duty or obligation do we have as community members to the people around us? Um, in the context that we've been talking about in context of mental wellness and community mental wellness,
In your opinion, I realized that you are one person.
[00:22:57] Melody: I am one person.
I don't know if this is too big, but if we truly believe that we are interconnected, that we're relatives, then let's examine how we treat one another. How do we share? What happens when we get into conflict, which is inevitable? How do we, do we tend to our Elders?
How do we tend to those that are sick? How do we tend to our children? Do we feel a sense of duty, um, to uplift one another? Or do we have this mindset of as long as I can take care of mine? I'm good.
I have a lot of learning to do there, um, because I internalize these colonial ideals that, um, and part of that is, um, immigrant trauma as well. This idea of scarcity, because we folks that have been displaced experience a lot of scarcity. And so there's a hoarding or saying what's mine is mine. What's yours is mine too, you know?
Um, That is trauma that requires healing, but how do we find healing in community when we start to practice differently, even if it's uncomfortable, even if, um, in that moment, it, um, doesn't seem to make sense in this capitalistic world.
I like to go into the place of reimagination. Of what do we imagine moving forward when as we, more and more of us join in to decolonize mental health care, what are the possibilities? And again, I'm just one person, so I can offer my slice of the pie, but it's a very, very, very, very big pie with many, many, many slices and flavors.
I'm imagining care that is integrated with our ways of being in our ways of living, that mental health care or mental health is not isolated to certain hours, like 50 minutes a week. That it is not isolated within the therapy room, that it is an integrative practice in how we, um, take care of our bodies, of our spirits, of the land, how we take care of one another.
I'm imagining that not only are we destigmatizing conversations about mental health, that we're celebrating conversations about mental health. That it, it's going beyond normalizing, but to uplift and to celebrate one another. Um, I'm imagining that, you know, each of us learn to feel a sense of duty and responsibility for one another's mental wellbeing. That this isn't something to just leave for the therapist. That your wellbeing is my responsibility as mine is to you
[00:26:26] Anne: that's a really great thought to end this on, actually, and I liked the idea of ending this with a bit of hope and possibility.
[00:26:38] Melody: Well, my name is Yang Hay, which means full of hope in Cantonese. Yup. So that is from my ancestors and I am gonna do my best to bring that into my relationships as well.
[00:26:56] Anne: You can follow Melody on Instagram at melody hope li, spelled L-I, and look for their work on Inclusive Therapists dot Com.
Just as Melody tries to bring hope to conversations around mental wellness and explore many different ways of healing, so does Ralph Sara through his podcast, The Anonymous Eskimo Recovery Podcast. His life was shaped in part by colonization and historical trauma, but he's actively working to help himself and others heal frothat
Ralph: My name is Ralph Sara. I was born and raised in Bethel, Alaska. Um, I am Yup’ik. I am Saami uh, you know, I'm a father, I'm a grandfather. I am, yeah, I'm a brother. I'm an uncle. So, um, that's who I am. I am a dental assistant by day, which means I have a full-time job, I work, you know, nine to five usually. And then I do my podcast.
Anne: So tell me a little bit about your podcast, the Anonymous Eskimo Recovery Podcast.
Ralph: Well, um, the reason that happened was I'm not too far out of treatment. It's been less than two years that I've been out of treatment. And while I was in treatment, I had a vision board that was in my room.
And, um, on that vision board was pictures of my family, of course, because that's what I wanted to get back was my children, uh, relationships with my children, relationships with my family. I also had material things like a house, you know, uh, a motorcycle and I had a cover of a book and the book was entitled “The Anonymous Eskimo.”
I was thinking to myself, you know, uh, books have a really big thing to do, you know, it would be awesome and it would be totally cool. But then as treatment went on, I was thinking other avenues, maybe I could do this, m I could do that, and a podcast, came up. So I Googled podcast after I got out, or not podcasts. I Googled Indigneous treatment, Indigneous recovery podcast. And there was zero out there. I could not find one. You find episodes, but not like a, a podcast totally for that. You know? And my podcast is not totally Indigneous, right. But I have like a soft focus on that. I tried to get as. Indigneous people on to share their stories, you know, for hope.
Anne: Tell me more about that. Like, why focus on Indigneous recovery? How is that different?
Ralph: Because I'm, you know, I'm Yup’ik? So, um, and the title of my podcast is Anonymous Eskimo, and that's my humor because, you know, nowadays Eskimo is a bad word, you know, it's frowned upon to say that, but when I was growing up, Eskimo was how I identified was Yup’ik Eskimo.
And, um, it wasn't a bad thing to be, Yup’ik Eskimo. I was proud of, you know, being a Yup’ik Eskimo. Um, but at the same time nowadays, it's kind of like, uh, oh, don't say that.
Being Native, I think, and having this podcast gives other people, other Native people, Indigneous people, kind of a voice that they'd never had before, because it was so frowned upon to talk about what you are going through. Talk about your traumas, talk about, you know, all the mental health things that happened to you before. You can't cry if you're a Native man, you know, you can't talk about things that are bothering you or hurting you. You have to be the strong stoic person, right?
That's how I was growing up. You know, it was, it was instilled upon you, you know, not in a way of schooling or anything. It was just like how you were brought up, you know, it was expected, I guess you could say.
The only thing I would witness was people getting drunk and then crying about it, crying about things that happen because that's the time that they, their emotions come out, you know?
And that's ultimately what, what became of me was that's how I learned how to deal with my pain and stuff like that. It was to get fricking plastered and then start crying about it, you know, or, you know, being angry and yelling about it, but you'd have to get drunk first, you know, to let it all out.
There's no healthy way of doing it. I was never taught that. I was only taught to hold it in. And, uh, and, and it was, it was okay to drink and let it out. Oh, he's just drunk, you know, he’s crying, letting out saying things that happened, whatever. Oh, he's drunk. So that's okay. Which unfortunately became normal, you know, Yeah.
That was a way of dealing with things. Unfortunately, when I was growing up
Anne: as an adult, have you kind of dug more into Yup'ik culture to figure out what used to be the ways
Ralph: Harold Napoleon wrote a great book about that. And, um, I, I've tried many times to get Harold Napoleon on my podcast and, um, having generational traumas and how that plays into that kind of the same thing, you know, you don't want to talk about that kind of stuff.
Um, you just hold it in, of all the things that happen before our generation, you know, all the deaths of, you know, the, the, the smallpox, you know, epidemic, whatever. Dealing with that, not being able to, uh, do your cultural activities, cultural dancing, and everything like that. Telling, um, either the Moravians or the Catholics or, you know, the Quakers, whichever part of Alaska that they divvied out to you to them or whatever, because we were, we were, um, Moravian in our area and, um, you know, they're telling you, you can't dance because it's demonic or whatever, you know, you can't have your, your, your t{I don’t understand what word he uses here}or markings or anything like that because that's, you know, they called us the heathens of the north.
So you're dealing with all of that generational trauma, and then you're adding all the, um, trauma that you've went through and you're still holding all of that in. You're going to let it out when you're drinking. Or that's the only way that you know, of letting it out, where you have to learn how to do it healthy in a, in a healthier way, which is so hard for people still.
Yeah.
Yeah.
Anne: It's hard to disassociate the history.
Ralph: And the stigma there's, there's no, you know, I think, I think there's always, always going to be that stigma of, you know, recovery,y being in recovery is a bad thing or, you know, the break, the stigma of the drunk Native, or, you know, or the drunk Indian, how they were portrayed and in movies and everything, or the drunk homeless guy that’s sitting out here on Spenard, you know, a lot of them are Native people,
So people have that stigma on there and that site in their mind. You know, those people they're experiencing their own trauma. They don't know how to deal with it.
Anne: Ralph said it took him a long time to deal with his own trauma. He went to treatment multiple times and even had long periods of sobriety. But it never really worked because he was doing it for someone else, like his family, and not for himself. That was until his most recent time in treatment when he was doing it because he wanted something different from his life.
Ralph: And so when I was in treatment, um, of course they have counselors there and this last time I was in treatment, you know, I, I decided to, you know, try to give it a try.
And I had a really great person. Her name was Bex Jacobs, shout out to her, but she got me to open up about things that I was so ashamed of and things that, um, I kept in and I didn't want to tell anybody, you know, I didn't want to tell my, my brother or my sisters or the closest people in my life, you know, I was so ashamed of doing all those things, uh, being a certain way, thinking a certain way, you know, it can eat at you. And that's a lot of the reason why people numb themselves with alcohol and drug addiction is, you know, they don't want to deal with that. They didn't want to think about it once you take that first drink or that, you know, hit of whatever, all that goes away, you're left with a numb feeling that, it feels awesome.
You know, so, yeah.
And I think a lot of it was, she got me to realize that past traumas or past things that I've, I've went through or things that I keep to myself, are a reason why I am redoing this over and over again. You know, I'm not done with drinking because I want to, every time I start to feel something, I want to numb that pain.
And if I don't deal with it in a healthy way, like talking to a clinician or using the tools that she has given me to kind of walk through this maze of emotions, I'll definitely fall back into that.
Getting out into nature is a big, you know, adventure therapy, she taught me
Anne: what's adventure therapy?
Ralph: Oh man. She had this adventure therapy class where we would go and hike or, you know, cross country ski one day a week at the treatment center where you go out there and we would talk during that, you know. She'd have her little sessions with people on the, on the hike trail or something like that, you know?
And then you get to be out there and just beautiful wilderness where some people, um, didn't think they'd be able to hike up a mountain and they did it. And they were like, oh my God, you know, look what I did, you know, and just being out there in Alaska’s beautiful country is just so it fills you with so, so much.
It gives you a time out there in the wilderness to be quiet and think about things too, you know, things that maybe happen during the week or, or during your lifetime, shoot, you know, it gives you time to process, which is, which is good.
Anne: It's very good.
Ralph: And, uh, and, and dealing with mental health, um, you have to have those avenues of, of releasing, you know, creative outlets, you know, be it music, you know, a hike on a mountain, writing down your thoughts, keeping a journal, whatever. Yeah. You know, let it out somehow; talking with a clinician.
Anne: For Ralph, his current primary outlet is his podcast, which helps many more people than just himself.
And that's another thing that's so needed is to have, have an outlet so other people know that they're not alone. You know, their, the way that they're thinking is they're so lonely, you know, because I don't know, being addicted to something or an alcoholic or whatever, it's just a lonely place to be. And having this podcast that I do shows other people that they're not alone, you know, there's so many different ways of people, um, achieving sobriety or recovery or, or even a better life, yknow. If they're doing something less than what they were doing before, like let's say somebody who's a heroin addict and now they're taking Suboxone or something, which is, you know, um, what do they call that? Harm reduction, harm reduction, you know, or, or like somebody who's an alcoholic, but they now, now they smoke a little weed or something like that, you know?
I think that's okay. You know, the way that you do. Is your way, you know, everybody is different, so everybody's gonna deal with their problem, different there's all these avenues that you can pick from. Yeah. Just like I was totally gung ho AA at first. And then I found my own way, you know, maybe helping people
Anne: Through the podcast instead of going to meetings?
Ralph: Through the podcast, you get to listen, listen to all these great people on here.
Courageous people, telling all their, you know, dark stories and funny stories and uplifting stories, you know? Um, a lot of it's sad and a lot of it's hurt and, but a lot of it's people rising up from the ashes of what they used to be to become these awesome people, you know,
Anne: Do you feel like that describes you, too?
Ralph: Um, you know, I've had periods of sobriety, right?
I've. I've fallen off the wagon so many times. I've had so many relapses. I've had long, long lengthy amounts of sobriety. I mean, months, years here and there, but I've always fell off. But I've never actually tried to help other people, you know, so maybe this is my way of having some kind of substance or just helping other people makes me feel good, you know, and just showing other people that it's not, it's not a, you can't be ashamed all the time, you know, don't be ashamed all the time. You've been through it, but you're not there anymore. And if you're going through it, yeah. There's ways to, to, to become a better person or have a better life, you know?
Anne: In Ralph's podcast, people share their own personal journeys and strategies for becoming better people. Many of the stories focus on Indigneous healing, such as this clip of Ralph's interview with Don Barnaby, a First Nations dancer from Quebec. He's telling the story of his first time dancing at a Pow Wow after becoming sober.
Don Barnaby: And I know that there was no wrong way to dance and that there is no right way to dance because, um, it's just a spirit that's out there dancing. No, our body is just a vessel that carries our spirit and that spirit was sober and alive and well, and it wanted to dance. So who was I tended to deny it, you know, and I went into that circle and I began to dance.
I don't know how I was dancing. Didn't matter. I just saw it was my spirit that was carrying me and it was. And then all of a sudden it started to pour and pour rain. You know when it started to rain everybody ran out of that circle, you know, and I kept on dancing. You know, and when the song was over, I came out of that circle, you know, and the drum was under the Arbor, so they were all safe and dry, you know?
So they, they started to sing again, you know. The rain had stopped when I left that circle. So when they came again and they started to sing another song, I turned around and I went back into that circle and started to dance. And once again, the rain came. And the rain came hard and it was just soaking me down to the bone, but I wasn't feeling it because, you know, like I said, it was, I was just a vessel that was carrying my spirit, you know?
And so after the song was over, I went to leave the circle and then they began another song, you know, and the rain had stopped and so I was like, oh, so I turned around again. And I went into that circle and it started to rain again. And then I began to realize that, you know, the Creator was, uh, washing away all my past and letting me know that, you know, I was being cleansed and it was okay.
And that from here on out that I could let my spirit free and just let it dance. And that it was a way like he was like forgiving me, you know, for everything that I'd done in the past. And then I realized, you know, all that medicine that I'd been looking for, I been searching for, I've been looking for in a bottle, looking for in a drug.
None of that medicine was good medicine for me, so it didn't allow me to heal. It was only mind altering, it wasn't spirit altering. So when I went into that circle and I heard that drum and I began to dance, that was the medicine that I was looking for my whole entire life.
Anne: In that clip, Don talked about dancing and healing. For Ralph, his podcast is a major part of his healing journey.
[00:16:10] Ralph: At this point in time in my life, um, I, I, I, I think I get more with doing this podcast and listening to other people's stories and how they did it and how they maintain their sobriety, you know, and what they, what they would say to other people still struggling. You know,
[00:16:34] Anne: It's almost like you've got a private AA group, uh, from around the world.
[00:16:38] Ralph: I've kind of thought I've kind of thought that before, like, Hey, you know, I know, you know, people are coming to me to, to tell their stories, which is totally awesome. Totally cool. And, uh, I, I'm just so thankful that I've been able to do this so far.
[00:16:54] Anne: Ralph Sara is the host of the Anonymous Eskimo Recovery Podcast. He's also one of the recipients of the Rasmusen 2021 Individual Artist Awards. He'll use the project funds to create an audiobook and music about his recovery journey. You can subscribe to his podcast pretty much anywhere. And you definitely should.
(music break)
During this episode we talked about a few ways to counteract the effects of colonization and white supremacy culture. We didn't even touch structural racism within psychiatry and how that leads to overdiagnosis and misdiagnosis of people of color or how other examples of systemic racism and discrimination affect mental health. We'll get there soon, I promise.
In the meantime, I want to keep this focus on hope. That’s what Melody left us with and what Ralph is doing with his podcast. Ralph said we need many different outlets for our thoughts and emotions.
I’d like to ask you to please take a moment to think about your outlets and ways you can help effect positive, equitable change. Maybe you could share your story, as Ralph does, or maybe you can consider ways you perpetuate white supremacy culture. If you’re in a safe space to do so, take a few breaths to ground yourself. Then grab a pencil and draw or write what your reimagined world looks like and how you can participate in bringing that to reality. Let it be a reminder that we all contribute to each other’s mental wellbeing.
This episode was edited by Susy Buchanan, produced by me, and includes theme music by Aria Philips. Our funding comes from the Alaska Center for Excellence in Journalism, the Alaska Mental Health Trust Authority, and the Alaska State Council of the Arts.
You can find more resources and other episodes at mentalhealthmosaics. org. Subscribe to this podcast and rate it on any podcast platform to help others find it. Thanks for listening and let’s stay hopeful.
[00:00:00] Anne: Welcome to Mental Health Mosaics, an exploration of mental health from Out North, which is located on the unceded traditional lands of the Dena'ina People in Anchorage, Alaska. I'm Anne Hillman.
On the last episode of Mental Health Mosaics we spoke about colonization, historical trauma, the intentional and ongoing destruction of Indigenous culture and identity, and how all of that relates to mental health. Yeah, it was a lot, and it was really only a fraction of all of the community-wide things we need to consider when talking about mental health.
And though we talked about the traumas that have long-term effects on communities, we also talked about the strengths and we touched very, very briefly on healing. -- Thanks, Meda! -- Never fear -- every episode of Mental Health Mosaics will also highlight ways to heal or move forward. Maybe that's in part because I'm annoyingly an eternal optimist and I'm the producer of this show, but mostly it's because there really are people who are striving to make the world better -- meaning more equitable -- for everyone.
In this episode I want to introduce you to two of those people. First is Melody Li.
[00:01:17] Melody: Hi everyone. My name is Melody Li and I use pronouns car in Cantonese and any in English. And I am a colony-born migrant, and a diasporic settler here on Turtle Island. I am a queer therapist of color. And also a mental health, um, liberation activist through our work in community at Inclusive Therapists.
[00:01:49] Anne: Melody is from Hong Kong and currently lives in Austin, Texas. I came across her work when I was trying to understand how mental health treatment is shaped by white supremacy culture. I know that some of you just flinched when I said those words. It's still something I'm getting used to saying in this context as well, and it’s a term that’s hotly debated. Is it useful? Divisive? Definitely a point of debate. Melody doesn’t actually use it in this conversation. She uses Eurocentric domination.
When I say white supremacy, I'm not talking about hate groups. Right now I’m not even talking about structural racism -- we’ll get to that in other episodes. I'm talking about how white ideas of what is right dominate our culture. These ideas are well laid out by Tem-uh O-kun in a whole website on white supremacy culture.
Think about the values that we often don’t even question, like individualism, perfectionism, and objectivity. This culture is why we primarily value knowledge when it comes with a degree or a published work, usually from a white-led institution. Many of us define success by gaining power and resources -- progress means getting bigger. White supremacist culture also defines professionalism by white standards and falls back on white-determined qualifications when promoting people in organizations. And it simplifies issues into either/or binaries -- you’re good or bad, that’s right or wrong. It doesn’t allow for nuances.
These ideas reign supreme and we all have them ingrained in us whether we want them to be or not. They originate in the creation of the United States which said white people should dominate all others, and they permeate well beyond our borders. There are links to many articles discussing these ideas on the Mental Health Mosaics website. Please check them out -- my explanation is limited because I’m still learning and I definitely welcome feedback. And I give many thanks to the folks at Native Movement who offer training that helped me start to notice this culture in ways I hadn’t before.
But back to Melody -- I sought them out because I wanted to learn from someone who is actively examining how white ideals shape what mental health treatment looks like and is advocating for change. They want to decolonize mental health, which means looking both at what happens in a therapy session and beyond. This is Melody:
[00:02:57] Melody: So we as a mental health field, um, dominate -- have a Eurocentric domination of what we consider to be valid. What we consider to be true knowledge or valid knowledge. And we gatekeep that through institutions of school, of our trainings of who gets to be licensed, who doesn't and which often not only neglects, but attempts to erase the lived experiences of Black Indigenous and people of color. And so it's a very limited knowledge base, but we try to pretend that these, this knowledge is universal because of colonial ideology.
Um, Another way that, um, coloniality shows up through the mental health field is the monopolizing of power through Eurocentric or American centric ontology, or how do we conceptualize what is reality? What is beinghood? What is personhood? What is humanity?
Anne: So I think I need a little bit more on that. Like... absolutely um, so one thing that we see often is, um, again for marginalized communities that may believe that one's being-hood is an interconnection with land, with non-humans, with animals, with plants, with water. These are our relatives. These are Indigenous practices here on Turtle Island, but also Indigenous, um, practices, um, across the globe.
And that our beinghood is also in interconnection with the spiritual, with the cosmos. Um, but, but when that is deemed um, not true through Eurocentric ontology, then we become quickly pathologized again. "Oh, this person, um, is dissociating." "This person doesn't have self-esteem or self-concept."
[00:05:11] Anne: Okay.
[00:05:12] Melody: Or when our reality is also, um, being questioned, um, there are folks that for example, may see visions or may hear, um, voices in interconnection with other beings. And when we are limited by Eurocentric ontology, then again, we pathologize and say, this person is. Um, we say all types of horrible, stigmatizing things, as opposed to saying, wow, there are actually different realities and different ways of being, and that is also a way that Eurocentric, um, psychology is very harmful.
[00:05:52] Anne: And so, seeing things just through a medicalized, Westernized system says things are wrong when really they're just not how other people experience life.
[00:06:04] Melody: Yes. Not how we experience and understand life. And so when I hear about stigma towards mental illness, how this is often used as blame on marginalized communities, especially, you know, Black, Indigenous, POC communities. We’re often blamed for not seeking mental health care. And we're often blamed to say, well, we, the people of color, stigmatize mental health and therapy, that's why they don't pursue it.
I always push back and I ask who stigmatized whom. That if we know that our ways of being and our realities and our understanding of personhood is not going to be honored and will be pathologized, that is a very risky situation to enter into.
And I can list so many examples. I come from a relatively collectivist culture, but when there's a Eurocentric lens that's put on our family models, our family systems, for example, we're often told that we are enmeshed. There's too much enmeshment. T here needs to be more individualism, um, self, self-concept, right? And this is actually really common and we're trained to look at what is wrong as opposed to valuing our ways of being. And this conceptualization is also very much interconnected with all the, what we call so-called phobias and isms, you know, gender binary, heteronormativity, um, fatphobia, classism, ableism. Christian centrism and all of this is embedded in the mental health field and we, we need to have a really honest and brave look at the ways that we are upholding this and are perpetuating harm through what we are selling as treatment or healing.
[00:08:31] Anne: You have used terms like decolonizing mental health. What does that mean?
[00:08:39] Melody: So Bhatia shares: it is about reclaiming water, land, territory, and language.
Decolonization means restoring what was lost.
That's where we start, because it's the water, land, language, culture, our ways of being that we're, that we're severed from that is the root of mental distress. So we're not starting with the symptoms. It's looking at what was lost and what is our role in the restoration. Um, restoration there is reparation.
Um, and, and for, for folks that have experienced colonization, this process is different from people that have inherited privilege through colonialism. Um, so for example, you know, in addition to land back, water back, that is always at the root, for, for simplicity’s sake, I'm going to say BIPOC or folks of color, for us it's all also about reclaiming our, our ways of being in our healing practices.
For folks that for example, may be descendants of colonial settlers, white colonial settlers, their work looks different. It means returning. Giving back. It means reparations. It means reorganizing, so now that we know that these hegemonic, you know, dominant, systemic, structures are in place. Those need to be dismantled.
And so there's, there are multiple processes, um, that happen simultaneously. Um, but if I were to simplify it, I would say, let's start with, um, focusing on, and this I'm learning from Indigenous communities, land back, Indigenous sovereignty and Black liberation. If the work that we do is not grounded in that, then there, we are always at risk of practicing in an exploitative manner, like something that is exploitive to communities of colors and Indigenous communities.
Um, and, and so in terms of the, how -- we got to do it in community. Because it's not something that can again be individualized. It's not a person saying, okay, I'm going to restructure my therapy practice and I'm going to read books because colonialism and coloniality. It's unfortunately embodied and also integrated in our mindsets.
And there, oftentimes we may not be aware of the ways that we can be oppressive, that we can be violent. And so being in community means that we, um, learn from one another, but also we, um, have systems of accountability that we talk about what rupture and repair means, that we look around corners from one another. We correct one another. And so I believe that decolonizing mental health care has to happen in community. And it's also a relational process between humans, but certainly. Non-humans and more than humans as well.
[00:12:31] Anne: And so and please, correct me if I'm wrong. I hear what you're saying in what you're saying, but it's not like we can just say, okay, let's do X, Y, or Z to mental health. To fix the mental healthcare system, we have to do it in concert with fixing all of these others systems. And that we need to do it while listening and making amends and accepting that that's going to look really different for everybody.
[00:13:02] Melody: Yes. It's going to look different depending on, gonna use that word, positionality, which means that we are made up of different social identities.
And some of our social identities hold more power. Some of our social identities may be marginalized and each of us have a unique combination or makeup of that. But when we look at our positionality, for example, some of my parts are, um, I have. Uh, skin color privilege. Um, I have non-disabled privilege. I have education and class background privilege.
However, there are other parts of me as I shared, um, my queerness, um, being a colony born person, being an immigrant. These are parts that are marginalized. I have to bring -- I'm bringing all of these parts in the work that I do in community. I bring all these parts also in the therapeutic setting. So I need to be mindful of not only my positionality, how I show up in relationships with others, but also in relations to this land. My position on this land is yes, I'm a diasporadic settler, but I'm a settler. This is not my land, so what is my responsibility as I'm on this land as a visitor, as a migrant, as a person seeking refuge?
That is different from someone with a different set of social identities that have a different relationship with this land. And, um, so, so that's why it's not really, um, possible to have an ABC because it requires us to bring our full beings in here, and these interactions are relational. At the same time, there are practical things we can do such as, um, learning, learning from Indigenous communities and writers and activists following their lead, following the lead of Black activists.
Um, and there's so much learning that we can do. And also I think an important part is healing. That if we're injured, if we have, um, injured through racialized trauma, or we have been, um, yeah, that even for white folks, when white folks were not always white folks. White folks belong somewhere, but when they are either displaced, um, or when they had to, um, not have to some chose to move away from their place of origin and give up their cultural identities, um, to trade in for power that, that there are ruptures there that happen as well. And that require healing because if we don't also, as practitioners focus on our healing, then we are more at risk of perpetuating, hurt, and harm and injuries on to others.
[00:16:27] Anne: So in this world where you're balancing these two things like your livelihood and seeing individual patients, as well as creating new structures, how do you bring this greater systemic work and this greater dismantling work into that individual practice? Like how are you trying to transition this Western model of sitting down one-on-one and talking to people into something that really is more inclusive and also more acknowledging just the reality of, of our intersectional identities in of our positionality.
[00:17:10] Melody: Um, the first thing that came to mind, I love this question is. I'm realizing that this is not on me, that my offerings are, are just, limited to what I, as one person can offer. So part of my work is to learn about, to connect with folks with different, um, ways of healing, different wellness practices, and being well resourced so that when a service user, you know, meets with me, I understand my limitations.
And this is something that we, as a field are, is not good at. That we, because in order to maintain power, we sell this image that we know at all, that we have all the answers, but actually what we need to know is our limitations. That my limitations are limited to my lived experiences, to my ancestral practices that may or may not be helpful for somebody else.
However, um, there are, I, I can hold space for someone I can, um, guide them to also look at their intergenerational lineage traumas. I can hold space for conversation about how oppression and a racialized violence impact them and their psyche and their relationships. So I can hold space for a lot of these relationships, these conversations, those dialogue, but I also need to be aware of different healing modalities that exist that can be helpful for them.
So that is one way. Another way is that, um, also creating these new systems of collective care that is not necessarily dependent on systems like insurance panels or, um, you know, capitalistic systems that are community funded. So that's something that our communities work really hard on. How do we extend care in a way um, honors the service users. And, um, and their needs, especially financial needs, but it's also, um, it's also sustaining to healers and therapists. So the work that I do, um, in the therapy room per se, it looks different during COVID is yes, we absolutely have one-on-one time. There is space for one-on-one time, but I am mindful that this, this 50 minutes I'm spending with this person once a week or every other week is only a slice of the possibilities of healing.
And can I offer them more? Um, and at the same time, am I also advocating for them outside of the therapy room?
[00:20:34] Anne: And it really highlights something that I feel like people are more and more realizing. Most people I've been speaking with are more and more realizing that like therapy in these conventional group therapy, individual therapy, these conventional ways that we've all been taught to seek help aren't the only ways. And seeking help by being part of a community garden, seeking help by just listening to people, seeking help through, you know, offering, offering food at a community fridge are always to also heal and be part of things.
[00:21:15] Melody: Yes, those are really the ways that, um, that get me excited that, um, because this mutual aid, um, is restorative to entire communities, not just the folks that are hurting. It's for all of us.
And so, so much more to this, and also reminding us that Mother Earth is so good to us, that there's so much healing that exists, that, you know, they so lovingly and generously offer us. But that we are not good stewards of,That through capitalism, we have disconnected from our, even are destroying. So part of our healing is also asking how do we return to a relationship, a respectful, loving, reciprocal relationship with Mother Earth. If the land is not well, if the water is not well, how can we possibly be mentally well?
[00:22:35] Anne: you say like we have this duty to the land around us, to the water around us. What sort of duty or obligation do we have as community members to the people around us? Um, in the context that we've been talking about in context of mental wellness and community mental wellness,
In your opinion, I realized that you are one person.
[00:22:57] Melody: I am one person.
I don't know if this is too big, but if we truly believe that we are interconnected, that we're relatives, then let's examine how we treat one another. How do we share? What happens when we get into conflict, which is inevitable? How do we, do we tend to our Elders?
How do we tend to those that are sick? How do we tend to our children? Do we feel a sense of duty, um, to uplift one another? Or do we have this mindset of as long as I can take care of mine? I'm good.
I have a lot of learning to do there, um, because I internalize these colonial ideals that, um, and part of that is, um, immigrant trauma as well. This idea of scarcity, because we folks that have been displaced experience a lot of scarcity. And so there's a hoarding or saying what's mine is mine. What's yours is mine too, you know?
Um, That is trauma that requires healing, but how do we find healing in community when we start to practice differently, even if it's uncomfortable, even if, um, in that moment, it, um, doesn't seem to make sense in this capitalistic world.
I like to go into the place of reimagination. Of what do we imagine moving forward when as we, more and more of us join in to decolonize mental health care, what are the possibilities? And again, I'm just one person, so I can offer my slice of the pie, but it's a very, very, very, very big pie with many, many, many slices and flavors.
I'm imagining care that is integrated with our ways of being in our ways of living, that mental health care or mental health is not isolated to certain hours, like 50 minutes a week. That it is not isolated within the therapy room, that it is an integrative practice in how we, um, take care of our bodies, of our spirits, of the land, how we take care of one another.
I'm imagining that not only are we destigmatizing conversations about mental health, that we're celebrating conversations about mental health. That it, it's going beyond normalizing, but to uplift and to celebrate one another. Um, I'm imagining that, you know, each of us learn to feel a sense of duty and responsibility for one another's mental wellbeing. That this isn't something to just leave for the therapist. That your wellbeing is my responsibility as mine is to you
[00:26:26] Anne: that's a really great thought to end this on, actually, and I liked the idea of ending this with a bit of hope and possibility.
[00:26:38] Melody: Well, my name is Yang Hay, which means full of hope in Cantonese. Yup. So that is from my ancestors and I am gonna do my best to bring that into my relationships as well.
[00:26:56] Anne: You can follow Melody on Instagram at melody hope li, spelled L-I, and look for their work on Inclusive Therapists dot Com.
Just as Melody tries to bring hope to conversations around mental wellness and explore many different ways of healing, so does Ralph Sara through his podcast, The Anonymous Eskimo Recovery Podcast. His life was shaped in part by colonization and historical trauma, but he's actively working to help himself and others heal frothat
Ralph: My name is Ralph Sara. I was born and raised in Bethel, Alaska. Um, I am Yup’ik. I am Saami uh, you know, I'm a father, I'm a grandfather. I am, yeah, I'm a brother. I'm an uncle. So, um, that's who I am. I am a dental assistant by day, which means I have a full-time job, I work, you know, nine to five usually. And then I do my podcast.
Anne: So tell me a little bit about your podcast, the Anonymous Eskimo Recovery Podcast.
Ralph: Well, um, the reason that happened was I'm not too far out of treatment. It's been less than two years that I've been out of treatment. And while I was in treatment, I had a vision board that was in my room.
And, um, on that vision board was pictures of my family, of course, because that's what I wanted to get back was my children, uh, relationships with my children, relationships with my family. I also had material things like a house, you know, uh, a motorcycle and I had a cover of a book and the book was entitled “The Anonymous Eskimo.”
I was thinking to myself, you know, uh, books have a really big thing to do, you know, it would be awesome and it would be totally cool. But then as treatment went on, I was thinking other avenues, maybe I could do this, m I could do that, and a podcast, came up. So I Googled podcast after I got out, or not podcasts. I Googled Indigneous treatment, Indigneous recovery podcast. And there was zero out there. I could not find one. You find episodes, but not like a, a podcast totally for that. You know? And my podcast is not totally Indigneous, right. But I have like a soft focus on that. I tried to get as. Indigneous people on to share their stories, you know, for hope.
Anne: Tell me more about that. Like, why focus on Indigneous recovery? How is that different?
Ralph: Because I'm, you know, I'm Yup’ik? So, um, and the title of my podcast is Anonymous Eskimo, and that's my humor because, you know, nowadays Eskimo is a bad word, you know, it's frowned upon to say that, but when I was growing up, Eskimo was how I identified was Yup’ik Eskimo.
And, um, it wasn't a bad thing to be, Yup’ik Eskimo. I was proud of, you know, being a Yup’ik Eskimo. Um, but at the same time nowadays, it's kind of like, uh, oh, don't say that.
Being Native, I think, and having this podcast gives other people, other Native people, Indigneous people, kind of a voice that they'd never had before, because it was so frowned upon to talk about what you are going through. Talk about your traumas, talk about, you know, all the mental health things that happened to you before. You can't cry if you're a Native man, you know, you can't talk about things that are bothering you or hurting you. You have to be the strong stoic person, right?
That's how I was growing up. You know, it was, it was instilled upon you, you know, not in a way of schooling or anything. It was just like how you were brought up, you know, it was expected, I guess you could say.
The only thing I would witness was people getting drunk and then crying about it, crying about things that happen because that's the time that they, their emotions come out, you know?
And that's ultimately what, what became of me was that's how I learned how to deal with my pain and stuff like that. It was to get fricking plastered and then start crying about it, you know, or, you know, being angry and yelling about it, but you'd have to get drunk first, you know, to let it all out.
There's no healthy way of doing it. I was never taught that. I was only taught to hold it in. And, uh, and, and it was, it was okay to drink and let it out. Oh, he's just drunk, you know, he’s crying, letting out saying things that happened, whatever. Oh, he's drunk. So that's okay. Which unfortunately became normal, you know, Yeah.
That was a way of dealing with things. Unfortunately, when I was growing up
Anne: as an adult, have you kind of dug more into Yup'ik culture to figure out what used to be the ways
Ralph: Harold Napoleon wrote a great book about that. And, um, I, I've tried many times to get Harold Napoleon on my podcast and, um, having generational traumas and how that plays into that kind of the same thing, you know, you don't want to talk about that kind of stuff.
Um, you just hold it in, of all the things that happen before our generation, you know, all the deaths of, you know, the, the, the smallpox, you know, epidemic, whatever. Dealing with that, not being able to, uh, do your cultural activities, cultural dancing, and everything like that. Telling, um, either the Moravians or the Catholics or, you know, the Quakers, whichever part of Alaska that they divvied out to you to them or whatever, because we were, we were, um, Moravian in our area and, um, you know, they're telling you, you can't dance because it's demonic or whatever, you know, you can't have your, your, your t{I don’t understand what word he uses here}or markings or anything like that because that's, you know, they called us the heathens of the north.
So you're dealing with all of that generational trauma, and then you're adding all the, um, trauma that you've went through and you're still holding all of that in. You're going to let it out when you're drinking. Or that's the only way that you know, of letting it out, where you have to learn how to do it healthy in a, in a healthier way, which is so hard for people still.
Yeah.
Yeah.
Anne: It's hard to disassociate the history.
Ralph: And the stigma there's, there's no, you know, I think, I think there's always, always going to be that stigma of, you know, recovery,y being in recovery is a bad thing or, you know, the break, the stigma of the drunk Native, or, you know, or the drunk Indian, how they were portrayed and in movies and everything, or the drunk homeless guy that’s sitting out here on Spenard, you know, a lot of them are Native people,
So people have that stigma on there and that site in their mind. You know, those people they're experiencing their own trauma. They don't know how to deal with it.
Anne: Ralph said it took him a long time to deal with his own trauma. He went to treatment multiple times and even had long periods of sobriety. But it never really worked because he was doing it for someone else, like his family, and not for himself. That was until his most recent time in treatment when he was doing it because he wanted something different from his life.
Ralph: And so when I was in treatment, um, of course they have counselors there and this last time I was in treatment, you know, I, I decided to, you know, try to give it a try.
And I had a really great person. Her name was Bex Jacobs, shout out to her, but she got me to open up about things that I was so ashamed of and things that, um, I kept in and I didn't want to tell anybody, you know, I didn't want to tell my, my brother or my sisters or the closest people in my life, you know, I was so ashamed of doing all those things, uh, being a certain way, thinking a certain way, you know, it can eat at you. And that's a lot of the reason why people numb themselves with alcohol and drug addiction is, you know, they don't want to deal with that. They didn't want to think about it once you take that first drink or that, you know, hit of whatever, all that goes away, you're left with a numb feeling that, it feels awesome.
You know, so, yeah.
And I think a lot of it was, she got me to realize that past traumas or past things that I've, I've went through or things that I keep to myself, are a reason why I am redoing this over and over again. You know, I'm not done with drinking because I want to, every time I start to feel something, I want to numb that pain.
And if I don't deal with it in a healthy way, like talking to a clinician or using the tools that she has given me to kind of walk through this maze of emotions, I'll definitely fall back into that.
Getting out into nature is a big, you know, adventure therapy, she taught me
Anne: what's adventure therapy?
Ralph: Oh man. She had this adventure therapy class where we would go and hike or, you know, cross country ski one day a week at the treatment center where you go out there and we would talk during that, you know. She'd have her little sessions with people on the, on the hike trail or something like that, you know?
And then you get to be out there and just beautiful wilderness where some people, um, didn't think they'd be able to hike up a mountain and they did it. And they were like, oh my God, you know, look what I did, you know, and just being out there in Alaska’s beautiful country is just so it fills you with so, so much.
It gives you a time out there in the wilderness to be quiet and think about things too, you know, things that maybe happen during the week or, or during your lifetime, shoot, you know, it gives you time to process, which is, which is good.
Anne: It's very good.
Ralph: And, uh, and, and dealing with mental health, um, you have to have those avenues of, of releasing, you know, creative outlets, you know, be it music, you know, a hike on a mountain, writing down your thoughts, keeping a journal, whatever. Yeah. You know, let it out somehow; talking with a clinician.
Anne: For Ralph, his current primary outlet is his podcast, which helps many more people than just himself.
And that's another thing that's so needed is to have, have an outlet so other people know that they're not alone. You know, their, the way that they're thinking is they're so lonely, you know, because I don't know, being addicted to something or an alcoholic or whatever, it's just a lonely place to be. And having this podcast that I do shows other people that they're not alone, you know, there's so many different ways of people, um, achieving sobriety or recovery or, or even a better life, yknow. If they're doing something less than what they were doing before, like let's say somebody who's a heroin addict and now they're taking Suboxone or something, which is, you know, um, what do they call that? Harm reduction, harm reduction, you know, or, or like somebody who's an alcoholic, but they now, now they smoke a little weed or something like that, you know?
I think that's okay. You know, the way that you do. Is your way, you know, everybody is different, so everybody's gonna deal with their problem, different there's all these avenues that you can pick from. Yeah. Just like I was totally gung ho AA at first. And then I found my own way, you know, maybe helping people
Anne: Through the podcast instead of going to meetings?
Ralph: Through the podcast, you get to listen, listen to all these great people on here.
Courageous people, telling all their, you know, dark stories and funny stories and uplifting stories, you know? Um, a lot of it's sad and a lot of it's hurt and, but a lot of it's people rising up from the ashes of what they used to be to become these awesome people, you know,
Anne: Do you feel like that describes you, too?
Ralph: Um, you know, I've had periods of sobriety, right?
I've. I've fallen off the wagon so many times. I've had so many relapses. I've had long, long lengthy amounts of sobriety. I mean, months, years here and there, but I've always fell off. But I've never actually tried to help other people, you know, so maybe this is my way of having some kind of substance or just helping other people makes me feel good, you know, and just showing other people that it's not, it's not a, you can't be ashamed all the time, you know, don't be ashamed all the time. You've been through it, but you're not there anymore. And if you're going through it, yeah. There's ways to, to, to become a better person or have a better life, you know?
Anne: In Ralph's podcast, people share their own personal journeys and strategies for becoming better people. Many of the stories focus on Indigneous healing, such as this clip of Ralph's interview with Don Barnaby, a First Nations dancer from Quebec. He's telling the story of his first time dancing at a Pow Wow after becoming sober.
Don Barnaby: And I know that there was no wrong way to dance and that there is no right way to dance because, um, it's just a spirit that's out there dancing. No, our body is just a vessel that carries our spirit and that spirit was sober and alive and well, and it wanted to dance. So who was I tended to deny it, you know, and I went into that circle and I began to dance.
I don't know how I was dancing. Didn't matter. I just saw it was my spirit that was carrying me and it was. And then all of a sudden it started to pour and pour rain. You know when it started to rain everybody ran out of that circle, you know, and I kept on dancing. You know, and when the song was over, I came out of that circle, you know, and the drum was under the Arbor, so they were all safe and dry, you know?
So they, they started to sing again, you know. The rain had stopped when I left that circle. So when they came again and they started to sing another song, I turned around and I went back into that circle and started to dance. And once again, the rain came. And the rain came hard and it was just soaking me down to the bone, but I wasn't feeling it because, you know, like I said, it was, I was just a vessel that was carrying my spirit, you know?
And so after the song was over, I went to leave the circle and then they began another song, you know, and the rain had stopped and so I was like, oh, so I turned around again. And I went into that circle and it started to rain again. And then I began to realize that, you know, the Creator was, uh, washing away all my past and letting me know that, you know, I was being cleansed and it was okay.
And that from here on out that I could let my spirit free and just let it dance. And that it was a way like he was like forgiving me, you know, for everything that I'd done in the past. And then I realized, you know, all that medicine that I'd been looking for, I been searching for, I've been looking for in a bottle, looking for in a drug.
None of that medicine was good medicine for me, so it didn't allow me to heal. It was only mind altering, it wasn't spirit altering. So when I went into that circle and I heard that drum and I began to dance, that was the medicine that I was looking for my whole entire life.
Anne: In that clip, Don talked about dancing and healing. For Ralph, his podcast is a major part of his healing journey.
[00:16:10] Ralph: At this point in time in my life, um, I, I, I, I think I get more with doing this podcast and listening to other people's stories and how they did it and how they maintain their sobriety, you know, and what they, what they would say to other people still struggling. You know,
[00:16:34] Anne: It's almost like you've got a private AA group, uh, from around the world.
[00:16:38] Ralph: I've kind of thought I've kind of thought that before, like, Hey, you know, I know, you know, people are coming to me to, to tell their stories, which is totally awesome. Totally cool. And, uh, I, I'm just so thankful that I've been able to do this so far.
[00:16:54] Anne: Ralph Sara is the host of the Anonymous Eskimo Recovery Podcast. He's also one of the recipients of the Rasmusen 2021 Individual Artist Awards. He'll use the project funds to create an audiobook and music about his recovery journey. You can subscribe to his podcast pretty much anywhere. And you definitely should.
(music break)
During this episode we talked about a few ways to counteract the effects of colonization and white supremacy culture. We didn't even touch structural racism within psychiatry and how that leads to overdiagnosis and misdiagnosis of people of color or how other examples of systemic racism and discrimination affect mental health. We'll get there soon, I promise.
In the meantime, I want to keep this focus on hope. That’s what Melody left us with and what Ralph is doing with his podcast. Ralph said we need many different outlets for our thoughts and emotions.
I’d like to ask you to please take a moment to think about your outlets and ways you can help effect positive, equitable change. Maybe you could share your story, as Ralph does, or maybe you can consider ways you perpetuate white supremacy culture. If you’re in a safe space to do so, take a few breaths to ground yourself. Then grab a pencil and draw or write what your reimagined world looks like and how you can participate in bringing that to reality. Let it be a reminder that we all contribute to each other’s mental wellbeing.
This episode was edited by Susy Buchanan, produced by me, and includes theme music by Aria Philips. Our funding comes from the Alaska Center for Excellence in Journalism, the Alaska Mental Health Trust Authority, and the Alaska State Council of the Arts.
You can find more resources and other episodes at mentalhealthmosaics. org. Subscribe to this podcast and rate it on any podcast platform to help others find it. Thanks for listening and let’s stay hopeful.
Racism
Racism and Mental Health
[00:00:00] Anne: Welcome to Mental Health Mosaics, an exploration of mental health from Out North, which is located on the unceded traditional lands of the Dena'ina People in Anchorage, Alaska. I'm Anne Hillman.
On this episode we're talking about racism and mental health, both racism within mental health systems and how racism in general affects mental health. We're talking about really painful stuff, like police brutality and misdiagnosis, so please care for yourself. Later in the episode, we'll also get into ways to shift the mental health system to start to solve the problems with psychiatrist and professor Dr. Ruth Shim.
We're starting this episode with another poem from M.C. MoHagani Magnetek, an African-American transwoman poet and activist, that speaks directly to police brutality, white supremacy, and pain. She puts all of these issues into context of her lived experience with mental health issues. Here's MoHagani:
[00:00:57] MoHagani: The title of this poem is “No Justice, George, No Peace Breonna,” clearly written in 2020.
Where are you now that George Floyd has died? Are you down and ready to ride? Take no more with your last breath? Let the system burn ‘till there’s, nothing left, but the hardcore reality that Black lives matter. Water cooler convo field with chatter, calling into question your humanity, like a grudge Corona, got a grip on sanity.
Got folks, sick, tired, hot bothered, and sad. Everybody. And their mama all pissed off and mad about a Black woman shot and killed in her own house. Don't act like you don't know Breonna Taylor's who I'm talking about. So, yeah, don't worry about that. Bucket of water. Remember the centuries of genocide and slaughter superiority complex can be unlearned.
And so what the roof is on fire, let it burn, give them, give them no choice, but to listen and respect our voice, get your hands out my pocket. No means no, we said stop it. Murderers getting paid on administrative leave promoted for using their needs to choke hope out of the people. All lives matter. Come on, man?
That shit ain't equal. Tell me what's making a difference supposed to look like. Match struck fireworks in broad daylight. No longer satiated refuse to be placated until the killing of our people ceases. If there's no justice for George and Breonna, there will be no peace.
[00:02:56] Anne: When we were talking about this episode of Mosaics and we're talking about, you know, mental health and oppression, like what made you think this poem? What about this poem made you associate it with mental health?
[00:03:09] MoHagani: Right. Well, you know, I think this, this episode's not just oppression, but we're talking about white supremacy.
We're talking about, um, structural institutionalized systemic internalized racism. There is, um, there's oppression and there is class issues, you know, police brutality, some serious things going on, right. But we must talk about these things and they like greatly affect every aspect of our lives. Racism and white supremacy are so invasive and not just how our lives access to healthcare, access to wealth access to, you know, to housing and, and, you know, treated fair fairly in the courts, but it impedes on our, on our own lives, you know? When you go home and like, you know, you're trying to mind your business, you know, just, just chilling, but you gotta, you know, watch, you know, catch the news clip or whatever, you know, now they got, what 11 white jurors and one, one Black juror on Ahmaud Arbery’s case, what's that about? Right. And I want to say, you know, attitudes have changed, maybe won't be so bad, but no, clearly there's a problem there, like what does that say? That message.
So it's just like hard, you know, you know, you can't like just come home and take racism off of you. Right. You just, you just can't go home and get rid of white supremacy because there's no food in the refrigerator. You know why you don't have any food? Is it? It's not always from my lack of trying.
It's the fact that, well, you can't get a job because they're not hiring Negroes today. Period. And that's that. And, and so, and this is like one hurdle after another one challenge after another, it impedes on our, on our personal relationships and the way we interact with one another, especially when we think about and talk about internalized racism, right?
So in, in, in this poem, I talked about superiority complex can't be unlearned. Well, just as, you know, European white Americans have been able to adopt this attitude that this superiority over people, you know, um, as people of color have often like, you know, internalized racism where we’re like inferior. Another word that I don't use, I don't use, but I can't say it is minority, right? There's nothing minor about me. Period. End of discussion on that. But, but to say that, that I’m minor I'm internalizing, it's like, I'm less than, and, and I'm not. So, and that plays into it, right. Internalized racism can, you know, make me like straighten my hair, perm my hair when my hair is like naturally curly, right? It’s kinky and stuff.
Internalized racism's like you see it in, in like many, uh, on a continent Africa, you go on African stores. I haven't seen here in, here in Anchorage. Yes, I have. I've seen them every place I've gone and gone to African stores to get traditional African food has always skin lightener there on the shelf somewhere, you know?
Right. So, you know, to lighten our skin to, to, to be more passable and, and you know, things, or one of the things that I remember, like learning, too, is like how you gonna interact with the police? Don't look them in the eye, you know, it'll say, cause you don't want to be confrontational, you know? And at one point in time in American history, you know, it's like if I'm walking down the street and there's some good, you know, old white folks walking, I had to like, you know, step off to the side and let them have the sidewalk that does what the days he was living in, you know, when we talk about segregation.
I'm not that old, I'll be 46 in January. I am. I am that old, right? I am that old, because I had my grandmother, I had my parents' memories and their experiences, how my grandmother's memories that I know of, right? Maybe things will start getting out of reach when I no longer have people like that to connect it, but then I still have the history books.
And I love history. So for me to like, you know, read about the past, I'm like experiencing this thing now.
[00:07:22] Anne: I mean, you tied directly to what Meda was talking about in the last episode where she was talking about how history reverberates through, and you're not disconnected in your, even if it's not in your living memory, it's still connected to you and the people around you.
[00:07:37] MoHagani: Totally, totally, totally. Like, you know, when, uh, what was it 2013? When I was like, you know, being discriminated against for using the ladies room at Humpy’s downtown. And, um, when I finally like, like left there and I was on my way home, I was like crying. I was like, how can this be? I've never been told where I can not go into.
I was never, I had never been discriminated against. I said, why is that? You know, it says, because like my ancestors, my African, African-American ancestors, like, you know, from. 1954 Plessy vs Board of Education, you know, the sixties and seventies, civil rights, man, you know, laid it all out on, on the line, just so I'm not like, you know, segregated against, you know, discriminated against, I can be in public situations.
You and I can use the same, like, ladies room, you know what I mean? Um, I can do those places. I had never, like, interacted, had to experience that type of discrimination in my lifetime. Now maybe, you know what I'm saying, job application or something like this that wasn't like overtly but then we, now we talking about this covert racism can, all those things factor into it.
Yeah. And you know, some things, some days I'd be like, wow, when I see the things that's happening in our world, right.
And I was like, man, this is like this, this post-George Floyd murder life is actually pretty good. You know, it's, it's sad that he had to, you know, he had to die. Breonna Taylor had to die, but there are things that are changing in our society, in our culture, in our attitudes and our mindsets. For the better.
[00:09:16] Anne: And you feel like that's holding true a year and a half later?
[00:09:19] MoHagani: Yeah. Yeah. I, I still think so. It's not just a trend, you know, trends, you know, cause like last time, you know, summer 2020 was nice. Nice. I didn't have to open any doors. You know what I'm saying? White folks would just like step out of the way, like, you know, hold the door open for me, you know, just to go into the, to the, to the grocery store.
I definitely see it a lot more in, uh, in the nonprofit world, in the arts world, there's, you know, more push to, you know, to, to get Black artists out there. It's more push for, you know, recognizing, uh, indigenous people and POCs.
You know, w we'll see, but I think the whole nation burning, the whole world burning, you know, summer 2020, like it really, really changed some things for us. So, but yeah, it's more, it's always more work to go.
You know, one more thing I say about racism that's important, too, is that it's a weapon that any, anyone can pick up and use at any given time. White folks do not have the monopoly on racism. Do not own a monopoly on racism. And I was like golly. I get into with some old Black folks, my friends and everything. They'd be like telling some old racist jokes about Chinese people or Japanese people. It's like, no, that's not cool, period.
Under no circumstances, we just, because we've internalized racism, we experience oppression don't mean you gotta turn around and treat other people like crap, period. Don't do it. You know? So those are the conversations that need to be had too. ‘Cause we, none of us are absolved from using this, you know.
Me personally, I've given it to characters in my stories, you know, it's like, I feel like saying some racist stuff, so I'm gonna put it on the character, like get it on out there for me, you know? But those attitudes are real and they’re genuine. And within our own cultures and language, we all have these very derogatory terms and names for other people, other cultures that they may not ever hear or know, because this is our own life language system. The only internal codes that we using, you know, da da da da, to speak ill about other folks.
But white folks don’t have the monopoly on racism and people need to learn to deal with that.
Um, but yeah, so, you know, in, in this piece, I've just like, you know, asking this question, where are we, where are we now?
You know, George Floyd has died as murder. Like what are we going to do next? You know, are you ready to, to like go and affect change in community, you know, help other people, uh, make our culture better, you know, community better by having these hard conversations on race in America, the hard conversations on, colonization, you know, don't, don't really want to talk about that.
But yeah, racism and white supremacy. It's a beast.
[00:12:11] Anne: Have you experienced that like in your treatment for, for mental illness? Have you experienced, like within the mental health system, people being white supremacists or being racist or just pushing ideas on you?
[00:12:30] MoHagani: Yeah. I mean, definitely received some stuff from, from, uh, patients that I was hospitalized with. You know, that's what, the thing that we, you know, we talk about mental, uh, health and being hospitalized. Oftentimes we talk about what it's like, you know, with the doctors and nurses and have been treated certain kinds of ways with them based on.
Um, and I that's it's, it's, it's difficult for me to say. Um, why people are discriminating against me sometimes. I dunno if it is because of race or because of gender, sometimes it's both. And, but I know it when I felt it, and I've had experienced quite a bit, a bit of that. Um, and I've been in a lot of different hospitals and, you know, Staten Island, um, Atlanta, Georgia, here in Anchorage, and I've been to every one but API.
You know, and so, uh, and I've been treated like, you know, sometimes in very, uh, disrespectful ways, neglectful ways, um, just this dismiss. Right? And like I remember this time where I had, um, a manic episode, I was, I was suicidal after being, um, kind of like, you know, just, just, I don't know what to say.
I, I want to say it was an attack was too strong, but this white man, basically, like he asked me was a woman or a man. And I says like, I have a dress on, I have these nails and have this lipstick on. I had black lipstick on that day and he grabs my head and he twists my head. So I can't tell your lipstick take apart from your face because you're Black, you know?
And then as I was moving away, he, you know, moves to like lifted up, my dress. And so when I called Alaska State Troopers about it, this was like 2017 around Labor Day. And. You know, and, and, you know, in, in when I call the trooper, it was like, yeah, I'm a look, you know, go, go, go check this out. Now my license has been changed, you know, to reflect that I'm female, my name is legally changed and everything.
So the officer was like, yeah, you know? Yes, ma'am. So he goes and talk to the other people to get their side of the story. So, but when he comes back and he's talking to me, he's like, misgendering me, what? You know, he's talking to me and it doesn't tell him. He says, well, this is a, it's a non-reportable crime.
Like what's a non-reportable crime. Basically, you're telling me what happened to me, a Black woman is not worth filling in some funky boxes. What happened to me wasn't worth that.
So when I'm and I'm hospitalized, you know, and I'm telling, you know, the, uh, the doctors and the nurses and the counselors, my experience of how, like, you know, this manic attack, this, this, this psychotic episode, this suicidal ideation stems from, you know, how I was treated, you know, racially discriminate against at Humpy’s racially attacked by, by, by this man here that, that plays into why I'm there in the hospital. Can they empathize with that? No, well, we don't know what to say, but you should definitely try this medication. See how you feel tomorrow. You know, that's just what it leads to. Cause you know, many of these doctors and physicians are not people of color, so they don't know what these experiences are like, you know, and how it actually factors into, uh, depression and, and, uh, and, and, and mania and panic and anxiety attacks, you know?
So yeah, that's like, you know, a major part, but I guess I started to say too, one of the things that they'll talk about is when you are hospitalized, you also are in there with other people who are, you know, going through some things.
However, they may have mental health issues, but they're still bringing themselves there. They’re still bringing their racist ideas. They still bring their transphobic ideas to the group, their homophobic ideas to the group, to the meetings, to the setting. And it's been taught, you know what I'm saying? It's like, yeah, you know, the counselors do the work in like setting these ground rules and stuff, but every now and then someone breaks these rules and says something very hurtful to another person. You know, why are you, why are you trying to get care and treatment? I just want to get, well, I don't want to have to, like, deal with no racism and transphobic stuff right now. You know, like, can I just be, you know, a patient?
But yeah, that's, that's my poem in the essence though, to, to, to speak to that. And to talk about, um, you know, specifically this one speaks to, you know, the deaths of Breonna Taylor and George Floyd. We’re talking about police brutality here. We talk about systems and we talking about like over four or 500 years of this captivity, like. And it's, it's, it's living with memory, you know what I'm saying? My great-grandma, grandmother, grandparents can, can tell me what it was like, you know, growing up as children and sharecropping that's, you know, it's not that far away.
MUSIC TRANSITION
That was MoHagani Magnetek talking about poetry, racism, and mental health. MoHagani's experiences are unfortunately not unique. Discrimination has a direct effect on mental health and there is discrimination and racism within the mental health system. To put MoHagani's experiences in a larger perspective I reached out to Dr. Ruth Shim, a Black psychiatrist who is working to fix these problems.
[00:18:12] Ruth: My name is Ruth Shim and I am a psychiatrist. Um, my official titles right now are that I am the Luke and Grace Kim professor in cultural psychiatry at the University of California, Davis, in the department of psychiatry and behavioral sciences. I'm also the associate Dean of diverse and inclusive education in the school of medicine at the University of California, Davis. Um, and so those are the, that's my day job. That's what I've been working on for the last couple of years. And, um, yeah, and I've been a psychiatrist for about, um, going on nearing, nearing 20 years now.
The work that I do is, has been really rewarding and, and I've managed to see a lot of, kind of the field of mental health. I see a lot of, um, what's wrong with, with mental health that particularly in this country, and that has led to me, um, trying to come up with solutions for how to fix some of the problems and the system as it relates to mental health.
[00:19:19] Anne: I really appreciate that about your work, that you're not just like, this is wrong and this is wrong, but this is where we go from here.
[00:19:26] Ruth: Yeah.
[00:19:27] Anne: How did you end up in psychiatry to begin with?
[00:19:31] Ruth: You know, it's interesting. I, for whatever reason, since I was really young, have always been interested in mental health and psychiatry, and I have no idea why, but I always tell people when I was like 10 or 11, I would read a Time Magazine articles about people with mental illnesses and I was always like, I remember there was a fascinating article in Time about, um, clozapine one of the, uh, drugs that treats schizophrenia and I read it cover to cover. And I found it so interesting and I was really young. And so I don't know where that interest comes from, but his, it has always been there for some reason.
Um, you know, as I have gotten older, um, clearly I've encountered lots of family members and friends that have struggled with mental health problems and substance use disorders. And so that kind of increased my interest, um, especially, um, the fact that. Uh, how those illnesses in my family and friends, how they were kind of not discussed all the time, how, how people kind of avoided the topic, uh and so that really led me to, to kind of strongly want to do something in the mental health world. Uh, I majored in psychology when I was in college and wanting to be a physician and decided to go to medical school and started out medical school, pretty certain that I was going to do psychiatry. And then, and then, um, somewhere in the middle of medical school started thinking that, um, Well, I had a lot of stigma about being a psychiatrist and the idea that people don't always view psychiatrists as like real doctors.
Um, and, and this idea that I was, you know, spending all this time and work to become this physician and to get this MD degree. And then, you know, to have people not know that I was an MD, I was like, can I spend the whole rest of my life? Um, having people not know that about me, like, you know, I'm, I'm working so hard.
Like I kind of want people to know like my efforts. And then, and then I did my psychiatry rotations as part of my medical school. Um, and I liked everything that I did in, in medicine, but I loved psychiatry. My psychiatry rotation. It was, it was just like the only rotation where I would wake up in the morning, like fully excited to, to just be at work and be interacting with patients.
And so I realized I needed to, um, not worry about any of those other concerns and just follow my passion.
ANNE: What do you think it was about being, like doing psychiatry that really just resonated with you?
Uh, I think that, um, It it's it's it's just to turn that question a little bit, you know, I, I think that people have a really strong perception of what a psychiatrist is.
There's like a, uh, an image of a psychiatrist and often it is like an older white man on a couch, um, you know, talking to a patient in, in his office. Um, and, and that is kind of the image of what a psychiatrist is. And I, um, you know, I, I just felt like there was more, um, there, there is more for what psychiatry should be.
And so I was kind of drawn to the idea that, that I wanted to change the perception of, of psychiatry and I wanted to change, um, how people view that field. Um, and, and really, because I think I was seeing so much, um, mental health problems everywhere, you know, like everyone is dealing with mental health problems.
Everyone is dealing with substance use disorders. This is, like, pervasive. And, and I didn't feel, I felt like the, the images of what a psychiatrist was were so removed from the day-to-day reality of what regular people are dealing with. And, and I really wanted to kind of think about how can we make this more accessible for people.
So that, that's one of the reasons I went into psychiatry because I wanted people to kind of look at me and say, oh, this is somebody that I could, um, go and see and talk to about my mental health problems. And maybe it's not like super expensive and maybe it's not so hard to access services. And maybe it's more about like trying to solve regular everyday problems that people have as, as it relates to mental health.
[00:24:02] Anne: I like your vision of what psychiatry could be.
[00:24:06] Ruth: Yeah. We're not there yet. We're not there yet, but I, I'm really encouraged because there's a lot of young people coming into the field that feel just like me and a lot of people that, um, have, have looked at the problems that we see in our society, the ways that so many people are having, um, uh, mental health issues, uh, and that they're not being addressed.
And, and how it's an equity issue in particular, how certain populations have less access to mental health services and substance use services and how, um, just the very nature of being oppressed and marginalized in society leads to, um, mental health problems, um, just by navigating the world when you're being discriminated against or when racism occurs.
And there are more and more people going into the field of psychiatry now that understand those things really clearly when that was never something that was highlighted, um, in traditional psychiatry training. So I'm really excited and hopeful for the future because I do think the field and the face of psychiatry is changing.
[00:25:16] Anne: That's really exciting to hear, because I mean, I fully admit that I come into it with the same biases of thinking, you know, you picture the New Yorker cartoon, and yeah, I don't view that as helpful. Whereas, like I talked to all these peer support specialists who have lived it, you know, and I'm like, oh yeah, you're the one I want to talk to.
[00:25:37] Ruth: Exactly. And that's the thing, you know, the, the other, um, perception that old perception of psychiatry is pretty elitist. Um, it's this idea that only certain people have expertise and everybody else should not be involved in the care or management of people with mental health issues. And so there is no space in that old model for peer specialists.
There's no space for psychologists. There's no space for social workers. And a large number of psychiatrists are still kind of like fighting. Fighting, um, other fields around prescribing rights, um, as if this is like the most critical issue that we have in the field of mental health. It's, you know, people do not access are not able to access mental health services.
And so if there are models that are trying to increase access, I, I don't understand why we spend so much time arguing and kind of excluding people from providing services and providing support, which is what many psychiatrists, uh, do. At least many psychiatrists of old do. And I, and I do I, again, one point out that I do think that coming into the field now and moving us in a new direction, there's a much more inclusive model for how psychiatry should be provided. There's much more thought that it should be done in teams, not this individual provider sitting on his couch, waiting for people to come in the office, but that teams, including peer specialists and psychologists and social workers and all number of people, work together to provide more population level care to people with mental health problems.
[00:27:18] Anne: That's, it's exciting to hear that you see that evolution happening.
Um, so let's take a step back and talk about where we were before we could talk about where we're going.
Um, I was, I was interested in talking to you because you were so open about talking about the inequities in mental health care, um, and how we got there. And I was wondering if, if you could talk about that place.
[00:27:45] Ruth: Yeah. So the reason that I'm so interested in inequities is because w the same as we talked about before, like the training that I got, and I got a great psychiatry training, and I had a great track psychiatry training experience, but that training involved, um, you know, providing the evidence-based treatments that we learn about to different populations. And I trained at Emory university. And one of the interesting things about Emory in Atlanta is that the training sites, there's two separate training sites. One site is at Emory University hospital, which is located distinctly in the suburbs of Atlanta, in the richest part of Atlanta.
Um, and then the other training site is Grady Memorial hospital, which is the poorest parts located in, in the city and downtown Atlanta in the poorest part of the city. And so you had these two sites and residents and trainees would rotate at both of these sites. And, um, what I started noticing kind of very early on in my training is that I'm the same provider. Um, and yet, and I'm doing the same thing. So I'm providing the exact same treatments and I'm talking to people exactly the same way and I'm prescribing the exact same, um, recommendations. And we're doing all of the same things around caring for these patients. But the outcomes for the people at Emory University hospital were completely different from the outcomes of people at Grady Memorial hospital.
And the difference was people for instance, with depression, when we, uh, when I would see them at Emory University hospital, I would treat them and we would prescribe medications and we would do therapy and they would get better. And then I would rotate at Grady Memorial hospital and do the exact same thing and they would not get better.
And, and I couldn't. I, I couldn't fundamentally understand, or I wanted to understand, what is happening here. Again, I'm, I'm no different, um, and the environments are different, but like, it's this, as, as many people have started, have posited, is there something about the population? Is there something intrinsic about the people at Grady Memorial hospital versus the people at Emory University hospital?
I couldn't figure it out. And one of the things that I remember thinking is the old models of, of education have really highlighted that those differences are the result of, um, biological or genetic differences between races and ethnicities or these differences are the result of cultural differences between, uh, racial and ethnic groups.
And none of that really made sense to me. And so that really started me on a journey where I started to understand that it's, it has very little to do with any of those things, and it has everything to do with the environment, um, with what we call the social determinants of health. Um, those factors where we live, learn, work and play that impact our health.
That these are the reasons why you see these huge differences and just the very, um, act of living in a neighborhood that is well-funded and well resourced versus living in a neighborhood that is underfunded. And under-resourced that those things can lead more significantly to differences in mental health outcomes.
Um, and those are the, and that's where we have to focus our interventions.
[00:31:24] Anne: So that seems completely logical to me. So why was that ever in question? Like why was that not ever just…
[00:31:36] Ruth: I take it, it's a great question. And, um, I think it's because, um, the people that have spent time in the field, um, did not have the experience of what it's like to be in a neighborhood to grow up in a neighborhood that is under-resourced and underfunded, um, or they didn't have the experience of, um, encountering, um, and, and interacting with people outside of that clinical environment, interacting with people that are from those under-resourced, um, and under funded neighborhoods.
And then, you know, there is this, this big, um, elephant in the room, which is structural racism, and it is so pervasive, this idea that our institutions have been built and created and, and have been, um, set up to advantage certain populations and certain racial and ethnic groups and disadvantage others.
And so that frame, um, medicine and psychiatry has operated in that frame since the beginning of time. Um, and so we, we have passed those values on, um, the idea that we look at a, um, an illness or we look at a condition and we say, um, that, that, that group has that condition because that group makes different choices, makes worse choices about their health or that group has that condition because that group, um, has a higher genetic predisposition to have this particular diagnosis or this particular problem, or, you know, even things like, uh, the, the belief that certain populations are more prone to use certain drugs um, uh, when, when that's, that's not been proven in any sort of way. So we've got all of these ideas and, and with that structurally racist frame that we all marinate in, in society, it's very easy to kind of err on the side of thinking that these differences have nothing to do with the social determinants and have everything to do with people's personal choices and individual decisions that they make.
[00:33:49] Anne: I feel like that's, that's a common, though less common than it used to be, story that's often told in Alaska, especially about Alaska Native people and, you know, indigenous people are more prone to being alcoholics when it's just…
[00:34:05] Ruth: That is one of, exactly, indigenous people and alcoholism is probably one of the most pervasive examples of mental health inequities um, in which many studies have been done, looking at genetic predisposition, um, to try and find the gene that exists among indigenous populations. So the gene that exists in Alaska Native populations that predicts higher rates of alcoholism with no understanding or consideration for the historical trauma that has been visited upon in indigenous populations since the founding of this country.
And the idea that, that historical trauma, that trauma, um, may in fact lead to, uh, through historical, um. uh., epigenetics may lead to gene changes, but really it is an environmental and a structural impact that leads to, um, uh, coping or a self-medication, um, through alcohol that is really driving this. And yet people want to say that this is some sort of biological or genetic, um, influence, or that again, Alaska Native populations, indigenous populations are somehow just, they like alcohol better, or they, or they make bad choices about, uh, about substances so they, they choose to use alcohol more, um, than other populations. And none of that is really accurate, but it has been very pervasive in, in our society.
[00:35:42] Anne: I have no medical doctors in my family who have told me these things when I first moved to Alaska and I was like, oh, they must know. I was like, okay.
And then you get up here and you start learning the true history. And it's like, oh, Everything, everything I've been taught is wrong. Are there, that's the most pervasive damaging lie? Are there other pervasive, um, assumptions made about Black populations are made about other, um, other cultural groups that pervade psychiatry that you're working to abolish?
[00:36:18] Ruth: Absolutely. And I think one of the clearest examples is, um, is thinking about schizophrenia and, um, the, the ways that we think about schizophrenia as it relates to Black people. Um, and so Jonathan, the author and psychiatrist, Jonathan Metzl wrote an incredible book on this called The Protest Psychosis: How Schizophrenia Became a Black Disease, and he really highlights how, um, in, in, around the 1960s, as we started to see the rise of the civil rights movement, the very definition of schizophrenia was kind of altered from this disease that mostly affected white women who were, um, not operating in their, um, uh, appropriate gender roles. So they weren't taking care of their households appropriately and they weren't cleaning and cooking, um, as much as they should have been and they would find themselves diagnosed with schizophrenia prior to the 1960s.
And then with the rise of the civil rights movement, um, you saw a shift and a definition of, uh, a type of psychosis called the protest psychosis where, um, schizophrenia was kind of reformed by psychiatry into this condition that was, um, that people were considered to be aggressive and hostile and violent and paranoid.
And, and that, um, really took off in the 60s and was really associated very particularly with Black, um, Black people and particularly Black men. Um, and so the very act of championing civil rights or the very act of trying to fight against, uh, oppression was mislabeled, um, in the minds of many white psychiatrists was mislabeled as a psychotic illness.
Um, and, and, and it's, it's really complicated because it's not even that it wasn't that there were, uh, there weren't some, there wasn't psychosis happening. So in some of those populations, there was a psychosis happening because stress induces psychosis. And so, um, those men and women that were fighting for civil rights were under higher levels of higher rates of stress and so they were in fact maybe some of them were having psychotic symptoms at times. But not because of the context by which it was defined and not because of the act itself of, of, of protesting and fighting for civil rights.
So what, what we saw in that time was really an erasure of context, a lack of understanding of how, um, the history, the socio-historical context by which somebody operates in, um, dictates their behavior and how behavior is, natural and normal behavior could be, pathologized to, to be seen as something, especially if you come from a place where you don't understand that context.
That behavior could be pathologized and, and, and attributed again, the hostility, the aggression. And, and so that happened in the sixties. And again, documented really well in the, in the book The Protests Psychosis, but that happened in the 60s. But what we have here in modern times, which has been really well studied by many researchers and could, including Steve Strakowski is that we see inequities in all sorts of outcomes, as it relates to, um, people of color and Black people and schizophrenia.
So Black people are more likely to be diagnosed with schizophrenia than with a mood disorder, like bipolar disorder or depression compared to white people. And, um, they're, they're, they're misdiagnosed, so they may have bipolar disorder and they're misdiagnosed as schizophrenia.
[00:40:08] Anne: Can you help me, um, I guess, understand the differences between these two diagnoses and kind of, yeah, understand the differences in why it matters if you're given one, versus the other, like with one student
[00:40:21] Ruth: matters a lot because of treatment options. And so when you have a mood condition, the treatment is a mood disorder. The treatment is often very different from a primary psychotic disorder.
And so, um, if you don't, if you're misdiagnosing the condition, you're often then providing the wrong treatment. Um, and so if somebody is not getting the most effective treatment for their condition, then they're not going to improve. And so, so what you see is in this particular population, a misdiagnosis followed by then, um, not the right, uh, management of symptoms, so a lack of improvement and then, um, you see these populations having again, worse outcomes.
So, so if you have misdiagnosed Black people, um, at higher rates, then those people do not recover completely from their illnesses. And then we look at like rates of, of, um, treatment responsiveness. And we say this particular population does not respond as well to this particular medicine or this particular therapy when really what it came down to was that the diagnosis was wrong in the first place.
Um, but even beyond making a mistake in the diagnosis, um, we also see things like, again, associated with this, this conceptualization of aggression, we see things like Black people are more likely to be put in seclusion and restraints. Um, when they go to the hospital for emergency psychiatric care, they're more likely so they're more likely to be seen as hostile and aggressive. They're more likely to be given, um, antipsychotic medications against their will to manage their behavior. Um, and they're more likely to be given higher doses of those antipsychotic medications. So, so the management, uh, in addition to the misdiagnosis, the management in crisis situations is, is more harmful.
Um, and like a very clear example I can give you is from my personal, um, clinical experience I've had, um, there, there are many different medications that you can use to treat psychotic symptoms. But one of the medications, an older medicine haloperidol is a medication that back in the 60s, um, when they were, uh, very strongly associating Black people with aggression and psychosis and schizophrenia, um, there were ads that you started to see, um, pop up in, um, psychiatric journals, which showed like a threatening aggressive Black man, um, and, and the, the headline on that ad the tagline on that ad set aggressive belligerent cooperation begins with Haldol. Um, and so what you've seen over time is that that particular medication somehow became associated in the minds of psychiatrists with that direct marketing with, oh, this is the medication you use when some, when a Black person presents with schizophrenia and is aggressive.
And so that marketing was very effective because, um, last year, one of my patients had to go into the hospital. Um, and I have, I have him on an antipsychotic medication and he was doing reasonably well, but then he had a, uh, a decline in his functioning. Um, and he went into the hospital and, um, he was hospitalized in a psychiatric facility.
And the first thing that the inpatient psychiatrist did was remove him from his medicine and start him on Haldol. And I thought to myself, why, why would, would that be the choice, the first choice, you know, and I, I certainly don't want to imply, um, that, that this, this inpatient psychiatrist was racist. Um, but I, but I also think there was a clear connection there because there is this connection in this drug that this drug works in this particular population.
It would be fine if that was a one-off thing, but a year later, uh, another patient of mine who is a Black woman, also went into the hospital because she had a decline in her functioning and she was taken off of her medication and put on Haldol. Now that being said, I have several white patients that when they go into the hospital, they are not put on Haldol.
So, so even today we see these inequities kind of, uh, and, and, and, you know, it's complicated because it's not like Haldol is a terrible medication. Um, but it has side effects and it has, and there are things to be considered, and it's not first-line anymore, really all the time for like ongoing outpatient management of schizophrenia.
And yet the only times that I've seen inpatient doctors prescribe that medication, um, to my patients is when they are, um, deemed to be aggressive or threatening or are, or when they're Black.
[00:45:28] Anne: Wow. Even today, it's like, it's not surprising and yet it's still
[00:45:35] Ruth: shocking. Even, even when it's not surprising, it's still shocking.
Anne: Yeah. Yeah. That's a really good distinction.
[00:45:46] Anne: So looking beyond like, these are heinous things to happen to individuals, but when you're treating individuals are not just looking at an individual, you've got a whole family and a whole community. How, how did these, um, how do these beliefs then spiral out wider into communities?
[00:46:08] Ruth: Um, I think that, I think that we, part of what happens is, as, so we, we are not, we are, we, human beings are not islands. And so we do not operate, um, independently. We operate within our family units. We operate within, um, our communities. Um, and I think that when one person has a negative interaction with the mental health um, system that scars families and communities.
Um, and, and, and again, um, so, so we know that, and I know from personal experience, you know, if you experienced discrimination, if you experienced mistreatment, when you go for, uh, services or care somewhere, um, I have never returned to a restaurant that I ate at where I felt I was discriminated against.
I've never once been like, okay, I'll go back there because it was probably a one-time. I always think I have choices, I have options, and I don't need to go to that restaurant again. Um, and so for mental health care, it's a little bit different. Um, people go and they're mistreated and they may be discriminated against in healthcare settings, um, and they then have very limited options about like, how, how do they re interface with that, um, with that setting. And so the damage that can be done, the damage that's done to one person, um, then ripples through that family. And so I spend a lot of time interacting clinically with family members who have been traumatized by watching their loved ones, be harmed, um, in seeking care, or be made to feel less than, or be, or be discriminated against in their pursuit of mental health care at maybe some of the worst times in that family's life when, when someone is in crisis and they need help and they're made to feel less than, and they're made to feel, um, not important and not valuable. Um, and so that then is, causes a ripple effect and then the whole family, um, and the whole community tends to kind of turn away from seeking those services.
And so that's when you end up with this narrative that certain populations, certain racial and ethnic groups, Black and Latinx populations, for example, indigenous populations that they, um, have so much stigma that they don't want to interact with the mental health system. And I'm not saying that stigma doesn't exist and I'm certainly not saying, um, no, there is no stigma, but I actually don't think that the driving factor in minoritized populations or populations that have traditionally been oppressed, I don't think it's actually stigma.
I think it's a very reasonable response to a system that has been harming individuals and a desire not to willingly interface with a system that has, that treats you like you're not worthy or is more likely to put you in seclusion and restraints when you go for crisis help. You know, I think that it's a very reasonable thing, not to want to interact with that system.
So it's not a stigma problem, as much as it's, uh, a general reasonable response to a trauma being elicited on you. And so then the, the, it's really important because the intervention is very different. So many times people say, oh, there's stigma in these particular populations. So we have to educate people on how important it is for them to seek mental health services and how important, and that is not where the emphasis needs to be.
The emphasis needs to be on us, improving the mental health system and to be providing, um, culturally humble services and structurally competent and structurally humble services that values and appreciates people and makes them feel, um, important and, and cared for. Um, and if we fix the system to be more trustworthy, then people will engage with the system more.
So it's not about educating. Um, it's not about educating certain populations and say, oh, you know, come, come to our health care system. If the onus is on the providers and the people in the healthcare system to make it a better place for people to enter.
[00:50:35] Anne: And you, you've done some work trying, like, talking about specific ways that could happen. What are specific ways? Like what, how can we make the mental health care treatment system actually responsive to people in a more inclusive? Not my, I hate the word inclusive,
[00:50:53] Ruth: I like the word inclusive.
[00:50:58] Anne: I think, I feel like I've encountered, oftentimes people are like, oh, let's make it inclusive, but they don't really,
[00:51:04] Ruth: there is no action following the inclusivity. Yeah, I hear you.
[00:51:09] Anne: So that's, I guess that's what I mean, like how do we make it like actually inclusive and mean it?
[00:51:16] Ruth: So I, I feel, I think there's many ways and I, um, but I, but I think that the lack of inclusivity and real action behind that inclusivity has to do mostly with power and power dynamics and who has power and who doesn't.
And so if we start to kind of like tease that apart, we see systems that are designed, um, to make it clear when people interface with those systems, that the people who have power are powerful, um, and that the people who don't are made to feel less than. And so then the work becomes unraveling that hierarchy that we have created within our mental health systems.
And that can happen on multiple levels. But I think the quickest way, the quickest way to get there is to have the people working in that system, be the very people, be the very people who are actively, um, from those communities and members of those communities.
That's when workforce diversity becomes most important because, um, because that is not the traditional ways that mental health clinics are designed. the mental health clinics do not traditionally reflect the demographics of the population that they're serving.
And so it, it really does. So it's not just a matter of, um, of, of creating a more diverse workforce. It's truly having the people that work in that particular mental health setting be from the very community that they're serving and look, and be those members of that community. And this is one of the reasons why I am so kind of supportive of the idea of peer specialists, because it is, it is, that is the very function of, of a peer specialist to be a person from the community who has lived experience, who knows exactly what it feels like to go through this situation and to be able to provide that care and support.
And that is the fastest way that we will make the settings, um, we, we will redesign these settings so that people can come in and feel valued and feel important because they are the setting. They are the people that are in that setting. And so that's the work that we have to do. Um, and that involves across all levels, um, aggressively diversifying the workforce.
Um, and we talk about workforce shortages and all of that, but I think we need more psychiatrists of color. We need more psychiatrists from oppressed and marginalized backgrounds. We need more sociologists and social workers and psychologists and peer specialists from, from all sorts of backgrounds.
Um, and that is the way that we, um, change, change the system and, and truly build an inclusive, um, mental health system.
[00:54:16] Anne: I'd like to delve a little bit more into, um, you kinda touched on people's lived experience and bringing that in and, and social determinants of health. Um, I'd love to kind of talk more about what can be done or what you're advocating people within the mental health field to do to really account for all of these other factors that influence our mental health, as opposed to just seeing a therapist or a psychiatrist.
[00:54:47] Ruth: I think one of the best ways that people can start to take action is by increasing awareness.
Um, and, and so I think that the mental health field, as it's kind of currently structured, spends a lot of time thinking about the individual patient that sits in front of, comes to the office and sits down in front of them. Um, and does an assessment that again, doesn't have all of the context in place and particularly the context that I think most providers miss when they do an evaluation on a, on a client or a person with a mental health problem is that they're missing the structural components.
They're missing that understanding of how those social determinants are interacting directly with that individual. So they're not understanding how, um, access to healthy foods or how poverty or how adverse childhood experiences or how homelessness or housing instability, um, they're not always understanding, uh, or how discrimination and racism and sexism, how they're not always understanding how those things show up in people's lives and they're not searching for it.
They're not asking questions about that. So they're not asking people about their identities. They're not trying to understand like who this person is and how the external world, um, has, has interacted with that person and who they are and who their identity is. Um, and I think that, uh, if, if we, as providers don't do that work, um, we're, we're dropping the ball on, on taking care of whole people and moving them towards health and wellness.
So, so the, the key, um, and the first step is recognizing that when somebody comes and sits in front of you, um, for an evaluation or for help, and, uh, in managing their mental health, that they're not just some diagnosis or they're not just some condition, but they are like a whole person who brings multiple identities and multiple, um, beliefs and, and, and multiple cultural, um, cultural identities to, to who they are and that, and that the job of the provider is to understand better that person's story and how they interact with the world and how the world interacts with that person.
So some people talk about this in the concept of structural competence. And this is again, um, Jonathan Metzl and Helena Hansen. This is work by Jonathan Metzl and Helena Hansen, um, to think about how we talk about cultural competence. We, we, we talk about how it's important to understand that there are lots of different cultures and understand the groups, um, that different cultures have different values.
But part of what structural competency is saying is we have to better understand how all of those social determinants show up in people's lives. And we have to be better at identifying those social determinants and asking people about those social determinants and thinking about that context.
[00:58:05] Anne: So to put this into terms that aren't using, like structural competency or social determinants, like basically helping providers, but potentially also helping individuals understand like all of the different factors that are happening around them and how that influences them from the stress of not having enough food to the stress of being discriminated against to the stress of having to navigate complicated systems that weren't built for you to navigate.
[00:58:39] Ruth: Exactly. Exactly.
[00:58:43] Anne: Making sure that I could explain this the way it's supposed to be. Explain it's it's
[00:58:46] Ruth: You explained it beautifully. And I think, um, that, that that's the key is, is that's not the model by which most psychiatrists are trained. Psychiatrists are trained to say, what are your symptoms? Um, you know, how much have you, you know, what's your appetite been like?
So like ask about appetite because appetite is a symptom of depression and poor appetite is a symptom of depression. Um, so ask if your appetite has changed, but not ask how, how, how easily can you access food? How easily can you access healthy foods? Um, do you have food insecurity?
And so there's like a number of the symptoms. So, uh, lack of sleep is, um, another symptom of depression. And so we ask those questions, how's your sleep, but we don't ask, um, is there like noise in your neighborhood that prevents you from sleeping? Is there, um, you know, are you witnessing violence or are you experiencing things that are interfering with your sleep that aren't just, I have this symptom of, of insomnia.
So it's really about it's, it's about going deeper and understanding how those environmental factors really do, um, come into play when, and we are social beings that interact with our environment. It seems pretty obvious, right?
Like we should be assessing how people interact with their environments and what's in those environments. Um, and that is just as critical as just understanding and ticking off the symptoms of certain disorders and conditions.
[01:00:19] Anne: This is going to sound like, like a really basic question, but I would love it if you could talk about, even just really quickly, like how discrimination directly affects mental health. Um, just so that people like grasp that.
[01:00:34] Ruth: Yeah. That's not a basic question at all. Um, uh, it's, it's a great, it's a great question. When, um, when I was working on, um, the book, the book, I edited, The Social Determinants of Mental Health, we were, um, trying to gather all those determinants and look at their impact on mental health outcomes. And there was this really fascinating pattern that we were just, uh, noticing when we were writing that book because we looked at things like discrimination, we looked at housing, we looked at food, we looked at adverse childhood experiences and there wasn't a lot of data out there at the time. And one of the things we noticed is that there was, um, a lot of data that showed, um, for almost all of those social determinants, there was a lot of data that showed, uh, that people, um, have significant physical health problems associated with things like adverse childhood experiences and housing instability and food insecurity.
Um, and there was less data to support that there were mental health impacts. We found them, but they were harder to find. And it was like that for all of the social determinants except discrimination. So for discrimination, there was not a lot of evidence to show that discrimination directly led to poor physical health, but there was an abundance of information and lots of data that showed that discrimination leads to poor mental health outcomes.
And specifically, certain diagnoses are directly correlated with being perceived as being discriminated against. So you actually don't even have to have been actively discriminated against. You, just as an individual, have to feel as if you were discriminated against. And that would lead to an increased risk of a number of mental health conditions, including major depressive disorder, alcohol use disorder, post-traumatic stress disorder, more days of having psychological distress, um, all of those illnesses, um, and all of those mental health conditions are tied directly to the experience of perceiving that you are discriminated against.
And so there's a direct line there. And again, it's really powerful because, um, that data is, is really robust data that we have on this. So absolutely discrimination leads to poor mental health and leads to poor mental health outcomes. And we have really strong data that scientists have been working on for, for decades now that that says that pretty definitively.
[01:03:15] Anne: And so the solution for that is?
[01:03:21] Ruth: Less discrimination. Less discrimination, I think is the key. How do we eliminate discrimination? Um, and, and so, you know, that, that leads a lot of people to say, okay, that's where we have to do implicit bias training. And I do think implicit bias training is one piece, but, but I also, again, I'm back to at least, you know, we can't solve discrimination in the world, you know, like that's too big of a, uh, a thing to address, but we can at least minimize the discrimination that people experience accessing healthcare.
Um, and there is, you know, um, David Williams is a researcher on, on racism and discrimination and health, and he created an everyday discrimination scale. And this is like a scale that asks people how they've been discriminated against in, in, in their lives. And this is where a lot of that data comes from that shows that if you score higher on that everyday discrimination scale, you have a greater likelihood of developing, um, a number of mental health conditions.
And, and one of the things that, uh, happened is that that everyday discrimination scale was adapted for health care settings. And so the same questions are now asked, has a nurse or doctor ever made you feel, um, that you were less than, or talk to you? Like you were, um, not important or, you know, made you feel like you were stupid.
Like those questions, um, that were part of the regular scale have now been adapted for the healthcare setting. So we can't fix all of the ills of society, but we could at least eliminate the discrimination that people experience when they go to seek health care and the discrimination that they experience when they get mental health care services.
And, and again, one of the quickest ways we can do that is by diversifying the workforce, by making sure that there are more people from those same identities providing care, because it's less likely that somebody is going to be discriminated against, by someone from the same group or category that they are in.
[01:05:25] Anne: Anything else you'd like to add before you run to your next meeting?
[01:05:29] Ruth: No, I just thank you so much for the time. It's been great to talk to you.
[01:05:33] Anne: Likewise. Thank you so much for your time.
That was Dr. Ruth Shim talking about racism and mental health. As Dr. Shim said, there are ways to make the mental health system more equitable. Part of that starts with diversifying the workforce and valuing the skills and life experiences that peer navigators bring to the table. Providers also need to consider all of the different aspects of life that influence our mental health, like the resources we have access to and the environment we live in.
During the next full episode of Mental Health Mosaics we'll delve more deeply into another issue that influences our mental health -- our sense of identity. You can find more resources related to all of these issues as well as poetry and art on our website, mental health mosaics -dot- org. If you enjoyed today's episode, help others find it by rating the podcast on any and all podcast platforms.
Today's episode was edited by Susy Buchanan with audio editing by Dave Waldron. Our theme music is by Aria Philips. I'm the show's host and producer. We received funding from the Alaska Center for Excellence in Journalism, the Alaska Mental Health Trust Authority, and the Alaska State Council for the Arts.
Thank you for listening!
[00:00:00] Anne: Welcome to Mental Health Mosaics, an exploration of mental health from Out North, which is located on the unceded traditional lands of the Dena'ina People in Anchorage, Alaska. I'm Anne Hillman.
On this episode we're talking about racism and mental health, both racism within mental health systems and how racism in general affects mental health. We're talking about really painful stuff, like police brutality and misdiagnosis, so please care for yourself. Later in the episode, we'll also get into ways to shift the mental health system to start to solve the problems with psychiatrist and professor Dr. Ruth Shim.
We're starting this episode with another poem from M.C. MoHagani Magnetek, an African-American transwoman poet and activist, that speaks directly to police brutality, white supremacy, and pain. She puts all of these issues into context of her lived experience with mental health issues. Here's MoHagani:
[00:00:57] MoHagani: The title of this poem is “No Justice, George, No Peace Breonna,” clearly written in 2020.
Where are you now that George Floyd has died? Are you down and ready to ride? Take no more with your last breath? Let the system burn ‘till there’s, nothing left, but the hardcore reality that Black lives matter. Water cooler convo field with chatter, calling into question your humanity, like a grudge Corona, got a grip on sanity.
Got folks, sick, tired, hot bothered, and sad. Everybody. And their mama all pissed off and mad about a Black woman shot and killed in her own house. Don't act like you don't know Breonna Taylor's who I'm talking about. So, yeah, don't worry about that. Bucket of water. Remember the centuries of genocide and slaughter superiority complex can be unlearned.
And so what the roof is on fire, let it burn, give them, give them no choice, but to listen and respect our voice, get your hands out my pocket. No means no, we said stop it. Murderers getting paid on administrative leave promoted for using their needs to choke hope out of the people. All lives matter. Come on, man?
That shit ain't equal. Tell me what's making a difference supposed to look like. Match struck fireworks in broad daylight. No longer satiated refuse to be placated until the killing of our people ceases. If there's no justice for George and Breonna, there will be no peace.
[00:02:56] Anne: When we were talking about this episode of Mosaics and we're talking about, you know, mental health and oppression, like what made you think this poem? What about this poem made you associate it with mental health?
[00:03:09] MoHagani: Right. Well, you know, I think this, this episode's not just oppression, but we're talking about white supremacy.
We're talking about, um, structural institutionalized systemic internalized racism. There is, um, there's oppression and there is class issues, you know, police brutality, some serious things going on, right. But we must talk about these things and they like greatly affect every aspect of our lives. Racism and white supremacy are so invasive and not just how our lives access to healthcare, access to wealth access to, you know, to housing and, and, you know, treated fair fairly in the courts, but it impedes on our, on our own lives, you know? When you go home and like, you know, you're trying to mind your business, you know, just, just chilling, but you gotta, you know, watch, you know, catch the news clip or whatever, you know, now they got, what 11 white jurors and one, one Black juror on Ahmaud Arbery’s case, what's that about? Right. And I want to say, you know, attitudes have changed, maybe won't be so bad, but no, clearly there's a problem there, like what does that say? That message.
So it's just like hard, you know, you know, you can't like just come home and take racism off of you. Right. You just, you just can't go home and get rid of white supremacy because there's no food in the refrigerator. You know why you don't have any food? Is it? It's not always from my lack of trying.
It's the fact that, well, you can't get a job because they're not hiring Negroes today. Period. And that's that. And, and so, and this is like one hurdle after another one challenge after another, it impedes on our, on our personal relationships and the way we interact with one another, especially when we think about and talk about internalized racism, right?
So in, in, in this poem, I talked about superiority complex can't be unlearned. Well, just as, you know, European white Americans have been able to adopt this attitude that this superiority over people, you know, um, as people of color have often like, you know, internalized racism where we’re like inferior. Another word that I don't use, I don't use, but I can't say it is minority, right? There's nothing minor about me. Period. End of discussion on that. But, but to say that, that I’m minor I'm internalizing, it's like, I'm less than, and, and I'm not. So, and that plays into it, right. Internalized racism can, you know, make me like straighten my hair, perm my hair when my hair is like naturally curly, right? It’s kinky and stuff.
Internalized racism's like you see it in, in like many, uh, on a continent Africa, you go on African stores. I haven't seen here in, here in Anchorage. Yes, I have. I've seen them every place I've gone and gone to African stores to get traditional African food has always skin lightener there on the shelf somewhere, you know?
Right. So, you know, to lighten our skin to, to, to be more passable and, and you know, things, or one of the things that I remember, like learning, too, is like how you gonna interact with the police? Don't look them in the eye, you know, it'll say, cause you don't want to be confrontational, you know? And at one point in time in American history, you know, it's like if I'm walking down the street and there's some good, you know, old white folks walking, I had to like, you know, step off to the side and let them have the sidewalk that does what the days he was living in, you know, when we talk about segregation.
I'm not that old, I'll be 46 in January. I am. I am that old, right? I am that old, because I had my grandmother, I had my parents' memories and their experiences, how my grandmother's memories that I know of, right? Maybe things will start getting out of reach when I no longer have people like that to connect it, but then I still have the history books.
And I love history. So for me to like, you know, read about the past, I'm like experiencing this thing now.
[00:07:22] Anne: I mean, you tied directly to what Meda was talking about in the last episode where she was talking about how history reverberates through, and you're not disconnected in your, even if it's not in your living memory, it's still connected to you and the people around you.
[00:07:37] MoHagani: Totally, totally, totally. Like, you know, when, uh, what was it 2013? When I was like, you know, being discriminated against for using the ladies room at Humpy’s downtown. And, um, when I finally like, like left there and I was on my way home, I was like crying. I was like, how can this be? I've never been told where I can not go into.
I was never, I had never been discriminated against. I said, why is that? You know, it says, because like my ancestors, my African, African-American ancestors, like, you know, from. 1954 Plessy vs Board of Education, you know, the sixties and seventies, civil rights, man, you know, laid it all out on, on the line, just so I'm not like, you know, segregated against, you know, discriminated against, I can be in public situations.
You and I can use the same, like, ladies room, you know what I mean? Um, I can do those places. I had never, like, interacted, had to experience that type of discrimination in my lifetime. Now maybe, you know what I'm saying, job application or something like this that wasn't like overtly but then we, now we talking about this covert racism can, all those things factor into it.
Yeah. And you know, some things, some days I'd be like, wow, when I see the things that's happening in our world, right.
And I was like, man, this is like this, this post-George Floyd murder life is actually pretty good. You know, it's, it's sad that he had to, you know, he had to die. Breonna Taylor had to die, but there are things that are changing in our society, in our culture, in our attitudes and our mindsets. For the better.
[00:09:16] Anne: And you feel like that's holding true a year and a half later?
[00:09:19] MoHagani: Yeah. Yeah. I, I still think so. It's not just a trend, you know, trends, you know, cause like last time, you know, summer 2020 was nice. Nice. I didn't have to open any doors. You know what I'm saying? White folks would just like step out of the way, like, you know, hold the door open for me, you know, just to go into the, to the, to the grocery store.
I definitely see it a lot more in, uh, in the nonprofit world, in the arts world, there's, you know, more push to, you know, to, to get Black artists out there. It's more push for, you know, recognizing, uh, indigenous people and POCs.
You know, w we'll see, but I think the whole nation burning, the whole world burning, you know, summer 2020, like it really, really changed some things for us. So, but yeah, it's more, it's always more work to go.
You know, one more thing I say about racism that's important, too, is that it's a weapon that any, anyone can pick up and use at any given time. White folks do not have the monopoly on racism. Do not own a monopoly on racism. And I was like golly. I get into with some old Black folks, my friends and everything. They'd be like telling some old racist jokes about Chinese people or Japanese people. It's like, no, that's not cool, period.
Under no circumstances, we just, because we've internalized racism, we experience oppression don't mean you gotta turn around and treat other people like crap, period. Don't do it. You know? So those are the conversations that need to be had too. ‘Cause we, none of us are absolved from using this, you know.
Me personally, I've given it to characters in my stories, you know, it's like, I feel like saying some racist stuff, so I'm gonna put it on the character, like get it on out there for me, you know? But those attitudes are real and they’re genuine. And within our own cultures and language, we all have these very derogatory terms and names for other people, other cultures that they may not ever hear or know, because this is our own life language system. The only internal codes that we using, you know, da da da da, to speak ill about other folks.
But white folks don’t have the monopoly on racism and people need to learn to deal with that.
Um, but yeah, so, you know, in, in this piece, I've just like, you know, asking this question, where are we, where are we now?
You know, George Floyd has died as murder. Like what are we going to do next? You know, are you ready to, to like go and affect change in community, you know, help other people, uh, make our culture better, you know, community better by having these hard conversations on race in America, the hard conversations on, colonization, you know, don't, don't really want to talk about that.
But yeah, racism and white supremacy. It's a beast.
[00:12:11] Anne: Have you experienced that like in your treatment for, for mental illness? Have you experienced, like within the mental health system, people being white supremacists or being racist or just pushing ideas on you?
[00:12:30] MoHagani: Yeah. I mean, definitely received some stuff from, from, uh, patients that I was hospitalized with. You know, that's what, the thing that we, you know, we talk about mental, uh, health and being hospitalized. Oftentimes we talk about what it's like, you know, with the doctors and nurses and have been treated certain kinds of ways with them based on.
Um, and I that's it's, it's, it's difficult for me to say. Um, why people are discriminating against me sometimes. I dunno if it is because of race or because of gender, sometimes it's both. And, but I know it when I felt it, and I've had experienced quite a bit, a bit of that. Um, and I've been in a lot of different hospitals and, you know, Staten Island, um, Atlanta, Georgia, here in Anchorage, and I've been to every one but API.
You know, and so, uh, and I've been treated like, you know, sometimes in very, uh, disrespectful ways, neglectful ways, um, just this dismiss. Right? And like I remember this time where I had, um, a manic episode, I was, I was suicidal after being, um, kind of like, you know, just, just, I don't know what to say.
I, I want to say it was an attack was too strong, but this white man, basically, like he asked me was a woman or a man. And I says like, I have a dress on, I have these nails and have this lipstick on. I had black lipstick on that day and he grabs my head and he twists my head. So I can't tell your lipstick take apart from your face because you're Black, you know?
And then as I was moving away, he, you know, moves to like lifted up, my dress. And so when I called Alaska State Troopers about it, this was like 2017 around Labor Day. And. You know, and, and, you know, in, in when I call the trooper, it was like, yeah, I'm a look, you know, go, go, go check this out. Now my license has been changed, you know, to reflect that I'm female, my name is legally changed and everything.
So the officer was like, yeah, you know? Yes, ma'am. So he goes and talk to the other people to get their side of the story. So, but when he comes back and he's talking to me, he's like, misgendering me, what? You know, he's talking to me and it doesn't tell him. He says, well, this is a, it's a non-reportable crime.
Like what's a non-reportable crime. Basically, you're telling me what happened to me, a Black woman is not worth filling in some funky boxes. What happened to me wasn't worth that.
So when I'm and I'm hospitalized, you know, and I'm telling, you know, the, uh, the doctors and the nurses and the counselors, my experience of how, like, you know, this manic attack, this, this, this psychotic episode, this suicidal ideation stems from, you know, how I was treated, you know, racially discriminate against at Humpy’s racially attacked by, by, by this man here that, that plays into why I'm there in the hospital. Can they empathize with that? No, well, we don't know what to say, but you should definitely try this medication. See how you feel tomorrow. You know, that's just what it leads to. Cause you know, many of these doctors and physicians are not people of color, so they don't know what these experiences are like, you know, and how it actually factors into, uh, depression and, and, uh, and, and, and mania and panic and anxiety attacks, you know?
So yeah, that's like, you know, a major part, but I guess I started to say too, one of the things that they'll talk about is when you are hospitalized, you also are in there with other people who are, you know, going through some things.
However, they may have mental health issues, but they're still bringing themselves there. They’re still bringing their racist ideas. They still bring their transphobic ideas to the group, their homophobic ideas to the group, to the meetings, to the setting. And it's been taught, you know what I'm saying? It's like, yeah, you know, the counselors do the work in like setting these ground rules and stuff, but every now and then someone breaks these rules and says something very hurtful to another person. You know, why are you, why are you trying to get care and treatment? I just want to get, well, I don't want to have to, like, deal with no racism and transphobic stuff right now. You know, like, can I just be, you know, a patient?
But yeah, that's, that's my poem in the essence though, to, to, to speak to that. And to talk about, um, you know, specifically this one speaks to, you know, the deaths of Breonna Taylor and George Floyd. We’re talking about police brutality here. We talk about systems and we talking about like over four or 500 years of this captivity, like. And it's, it's, it's living with memory, you know what I'm saying? My great-grandma, grandmother, grandparents can, can tell me what it was like, you know, growing up as children and sharecropping that's, you know, it's not that far away.
MUSIC TRANSITION
That was MoHagani Magnetek talking about poetry, racism, and mental health. MoHagani's experiences are unfortunately not unique. Discrimination has a direct effect on mental health and there is discrimination and racism within the mental health system. To put MoHagani's experiences in a larger perspective I reached out to Dr. Ruth Shim, a Black psychiatrist who is working to fix these problems.
[00:18:12] Ruth: My name is Ruth Shim and I am a psychiatrist. Um, my official titles right now are that I am the Luke and Grace Kim professor in cultural psychiatry at the University of California, Davis, in the department of psychiatry and behavioral sciences. I'm also the associate Dean of diverse and inclusive education in the school of medicine at the University of California, Davis. Um, and so those are the, that's my day job. That's what I've been working on for the last couple of years. And, um, yeah, and I've been a psychiatrist for about, um, going on nearing, nearing 20 years now.
The work that I do is, has been really rewarding and, and I've managed to see a lot of, kind of the field of mental health. I see a lot of, um, what's wrong with, with mental health that particularly in this country, and that has led to me, um, trying to come up with solutions for how to fix some of the problems and the system as it relates to mental health.
[00:19:19] Anne: I really appreciate that about your work, that you're not just like, this is wrong and this is wrong, but this is where we go from here.
[00:19:26] Ruth: Yeah.
[00:19:27] Anne: How did you end up in psychiatry to begin with?
[00:19:31] Ruth: You know, it's interesting. I, for whatever reason, since I was really young, have always been interested in mental health and psychiatry, and I have no idea why, but I always tell people when I was like 10 or 11, I would read a Time Magazine articles about people with mental illnesses and I was always like, I remember there was a fascinating article in Time about, um, clozapine one of the, uh, drugs that treats schizophrenia and I read it cover to cover. And I found it so interesting and I was really young. And so I don't know where that interest comes from, but his, it has always been there for some reason.
Um, you know, as I have gotten older, um, clearly I've encountered lots of family members and friends that have struggled with mental health problems and substance use disorders. And so that kind of increased my interest, um, especially, um, the fact that. Uh, how those illnesses in my family and friends, how they were kind of not discussed all the time, how, how people kind of avoided the topic, uh and so that really led me to, to kind of strongly want to do something in the mental health world. Uh, I majored in psychology when I was in college and wanting to be a physician and decided to go to medical school and started out medical school, pretty certain that I was going to do psychiatry. And then, and then, um, somewhere in the middle of medical school started thinking that, um, Well, I had a lot of stigma about being a psychiatrist and the idea that people don't always view psychiatrists as like real doctors.
Um, and, and this idea that I was, you know, spending all this time and work to become this physician and to get this MD degree. And then, you know, to have people not know that I was an MD, I was like, can I spend the whole rest of my life? Um, having people not know that about me, like, you know, I'm, I'm working so hard.
Like I kind of want people to know like my efforts. And then, and then I did my psychiatry rotations as part of my medical school. Um, and I liked everything that I did in, in medicine, but I loved psychiatry. My psychiatry rotation. It was, it was just like the only rotation where I would wake up in the morning, like fully excited to, to just be at work and be interacting with patients.
And so I realized I needed to, um, not worry about any of those other concerns and just follow my passion.
ANNE: What do you think it was about being, like doing psychiatry that really just resonated with you?
Uh, I think that, um, It it's it's it's just to turn that question a little bit, you know, I, I think that people have a really strong perception of what a psychiatrist is.
There's like a, uh, an image of a psychiatrist and often it is like an older white man on a couch, um, you know, talking to a patient in, in his office. Um, and, and that is kind of the image of what a psychiatrist is. And I, um, you know, I, I just felt like there was more, um, there, there is more for what psychiatry should be.
And so I was kind of drawn to the idea that, that I wanted to change the perception of, of psychiatry and I wanted to change, um, how people view that field. Um, and, and really, because I think I was seeing so much, um, mental health problems everywhere, you know, like everyone is dealing with mental health problems.
Everyone is dealing with substance use disorders. This is, like, pervasive. And, and I didn't feel, I felt like the, the images of what a psychiatrist was were so removed from the day-to-day reality of what regular people are dealing with. And, and I really wanted to kind of think about how can we make this more accessible for people.
So that, that's one of the reasons I went into psychiatry because I wanted people to kind of look at me and say, oh, this is somebody that I could, um, go and see and talk to about my mental health problems. And maybe it's not like super expensive and maybe it's not so hard to access services. And maybe it's more about like trying to solve regular everyday problems that people have as, as it relates to mental health.
[00:24:02] Anne: I like your vision of what psychiatry could be.
[00:24:06] Ruth: Yeah. We're not there yet. We're not there yet, but I, I'm really encouraged because there's a lot of young people coming into the field that feel just like me and a lot of people that, um, have, have looked at the problems that we see in our society, the ways that so many people are having, um, uh, mental health issues, uh, and that they're not being addressed.
And, and how it's an equity issue in particular, how certain populations have less access to mental health services and substance use services and how, um, just the very nature of being oppressed and marginalized in society leads to, um, mental health problems, um, just by navigating the world when you're being discriminated against or when racism occurs.
And there are more and more people going into the field of psychiatry now that understand those things really clearly when that was never something that was highlighted, um, in traditional psychiatry training. So I'm really excited and hopeful for the future because I do think the field and the face of psychiatry is changing.
[00:25:16] Anne: That's really exciting to hear, because I mean, I fully admit that I come into it with the same biases of thinking, you know, you picture the New Yorker cartoon, and yeah, I don't view that as helpful. Whereas, like I talked to all these peer support specialists who have lived it, you know, and I'm like, oh yeah, you're the one I want to talk to.
[00:25:37] Ruth: Exactly. And that's the thing, you know, the, the other, um, perception that old perception of psychiatry is pretty elitist. Um, it's this idea that only certain people have expertise and everybody else should not be involved in the care or management of people with mental health issues. And so there is no space in that old model for peer specialists.
There's no space for psychologists. There's no space for social workers. And a large number of psychiatrists are still kind of like fighting. Fighting, um, other fields around prescribing rights, um, as if this is like the most critical issue that we have in the field of mental health. It's, you know, people do not access are not able to access mental health services.
And so if there are models that are trying to increase access, I, I don't understand why we spend so much time arguing and kind of excluding people from providing services and providing support, which is what many psychiatrists, uh, do. At least many psychiatrists of old do. And I, and I do I, again, one point out that I do think that coming into the field now and moving us in a new direction, there's a much more inclusive model for how psychiatry should be provided. There's much more thought that it should be done in teams, not this individual provider sitting on his couch, waiting for people to come in the office, but that teams, including peer specialists and psychologists and social workers and all number of people, work together to provide more population level care to people with mental health problems.
[00:27:18] Anne: That's, it's exciting to hear that you see that evolution happening.
Um, so let's take a step back and talk about where we were before we could talk about where we're going.
Um, I was, I was interested in talking to you because you were so open about talking about the inequities in mental health care, um, and how we got there. And I was wondering if, if you could talk about that place.
[00:27:45] Ruth: Yeah. So the reason that I'm so interested in inequities is because w the same as we talked about before, like the training that I got, and I got a great psychiatry training, and I had a great track psychiatry training experience, but that training involved, um, you know, providing the evidence-based treatments that we learn about to different populations. And I trained at Emory university. And one of the interesting things about Emory in Atlanta is that the training sites, there's two separate training sites. One site is at Emory University hospital, which is located distinctly in the suburbs of Atlanta, in the richest part of Atlanta.
Um, and then the other training site is Grady Memorial hospital, which is the poorest parts located in, in the city and downtown Atlanta in the poorest part of the city. And so you had these two sites and residents and trainees would rotate at both of these sites. And, um, what I started noticing kind of very early on in my training is that I'm the same provider. Um, and yet, and I'm doing the same thing. So I'm providing the exact same treatments and I'm talking to people exactly the same way and I'm prescribing the exact same, um, recommendations. And we're doing all of the same things around caring for these patients. But the outcomes for the people at Emory University hospital were completely different from the outcomes of people at Grady Memorial hospital.
And the difference was people for instance, with depression, when we, uh, when I would see them at Emory University hospital, I would treat them and we would prescribe medications and we would do therapy and they would get better. And then I would rotate at Grady Memorial hospital and do the exact same thing and they would not get better.
And, and I couldn't. I, I couldn't fundamentally understand, or I wanted to understand, what is happening here. Again, I'm, I'm no different, um, and the environments are different, but like, it's this, as, as many people have started, have posited, is there something about the population? Is there something intrinsic about the people at Grady Memorial hospital versus the people at Emory University hospital?
I couldn't figure it out. And one of the things that I remember thinking is the old models of, of education have really highlighted that those differences are the result of, um, biological or genetic differences between races and ethnicities or these differences are the result of cultural differences between, uh, racial and ethnic groups.
And none of that really made sense to me. And so that really started me on a journey where I started to understand that it's, it has very little to do with any of those things, and it has everything to do with the environment, um, with what we call the social determinants of health. Um, those factors where we live, learn, work and play that impact our health.
That these are the reasons why you see these huge differences and just the very, um, act of living in a neighborhood that is well-funded and well resourced versus living in a neighborhood that is underfunded. And under-resourced that those things can lead more significantly to differences in mental health outcomes.
Um, and those are the, and that's where we have to focus our interventions.
[00:31:24] Anne: So that seems completely logical to me. So why was that ever in question? Like why was that not ever just…
[00:31:36] Ruth: I take it, it's a great question. And, um, I think it's because, um, the people that have spent time in the field, um, did not have the experience of what it's like to be in a neighborhood to grow up in a neighborhood that is under-resourced and underfunded, um, or they didn't have the experience of, um, encountering, um, and, and interacting with people outside of that clinical environment, interacting with people that are from those under-resourced, um, and under funded neighborhoods.
And then, you know, there is this, this big, um, elephant in the room, which is structural racism, and it is so pervasive, this idea that our institutions have been built and created and, and have been, um, set up to advantage certain populations and certain racial and ethnic groups and disadvantage others.
And so that frame, um, medicine and psychiatry has operated in that frame since the beginning of time. Um, and so we, we have passed those values on, um, the idea that we look at a, um, an illness or we look at a condition and we say, um, that, that, that group has that condition because that group makes different choices, makes worse choices about their health or that group has that condition because that group, um, has a higher genetic predisposition to have this particular diagnosis or this particular problem, or, you know, even things like, uh, the, the belief that certain populations are more prone to use certain drugs um, uh, when, when that's, that's not been proven in any sort of way. So we've got all of these ideas and, and with that structurally racist frame that we all marinate in, in society, it's very easy to kind of err on the side of thinking that these differences have nothing to do with the social determinants and have everything to do with people's personal choices and individual decisions that they make.
[00:33:49] Anne: I feel like that's, that's a common, though less common than it used to be, story that's often told in Alaska, especially about Alaska Native people and, you know, indigenous people are more prone to being alcoholics when it's just…
[00:34:05] Ruth: That is one of, exactly, indigenous people and alcoholism is probably one of the most pervasive examples of mental health inequities um, in which many studies have been done, looking at genetic predisposition, um, to try and find the gene that exists among indigenous populations. So the gene that exists in Alaska Native populations that predicts higher rates of alcoholism with no understanding or consideration for the historical trauma that has been visited upon in indigenous populations since the founding of this country.
And the idea that, that historical trauma, that trauma, um, may in fact lead to, uh, through historical, um. uh., epigenetics may lead to gene changes, but really it is an environmental and a structural impact that leads to, um, uh, coping or a self-medication, um, through alcohol that is really driving this. And yet people want to say that this is some sort of biological or genetic, um, influence, or that again, Alaska Native populations, indigenous populations are somehow just, they like alcohol better, or they, or they make bad choices about, uh, about substances so they, they choose to use alcohol more, um, than other populations. And none of that is really accurate, but it has been very pervasive in, in our society.
[00:35:42] Anne: I have no medical doctors in my family who have told me these things when I first moved to Alaska and I was like, oh, they must know. I was like, okay.
And then you get up here and you start learning the true history. And it's like, oh, Everything, everything I've been taught is wrong. Are there, that's the most pervasive damaging lie? Are there other pervasive, um, assumptions made about Black populations are made about other, um, other cultural groups that pervade psychiatry that you're working to abolish?
[00:36:18] Ruth: Absolutely. And I think one of the clearest examples is, um, is thinking about schizophrenia and, um, the, the ways that we think about schizophrenia as it relates to Black people. Um, and so Jonathan, the author and psychiatrist, Jonathan Metzl wrote an incredible book on this called The Protest Psychosis: How Schizophrenia Became a Black Disease, and he really highlights how, um, in, in, around the 1960s, as we started to see the rise of the civil rights movement, the very definition of schizophrenia was kind of altered from this disease that mostly affected white women who were, um, not operating in their, um, uh, appropriate gender roles. So they weren't taking care of their households appropriately and they weren't cleaning and cooking, um, as much as they should have been and they would find themselves diagnosed with schizophrenia prior to the 1960s.
And then with the rise of the civil rights movement, um, you saw a shift and a definition of, uh, a type of psychosis called the protest psychosis where, um, schizophrenia was kind of reformed by psychiatry into this condition that was, um, that people were considered to be aggressive and hostile and violent and paranoid.
And, and that, um, really took off in the 60s and was really associated very particularly with Black, um, Black people and particularly Black men. Um, and so the very act of championing civil rights or the very act of trying to fight against, uh, oppression was mislabeled, um, in the minds of many white psychiatrists was mislabeled as a psychotic illness.
Um, and, and, and it's, it's really complicated because it's not even that it wasn't that there were, uh, there weren't some, there wasn't psychosis happening. So in some of those populations, there was a psychosis happening because stress induces psychosis. And so, um, those men and women that were fighting for civil rights were under higher levels of higher rates of stress and so they were in fact maybe some of them were having psychotic symptoms at times. But not because of the context by which it was defined and not because of the act itself of, of, of protesting and fighting for civil rights.
So what, what we saw in that time was really an erasure of context, a lack of understanding of how, um, the history, the socio-historical context by which somebody operates in, um, dictates their behavior and how behavior is, natural and normal behavior could be, pathologized to, to be seen as something, especially if you come from a place where you don't understand that context.
That behavior could be pathologized and, and, and attributed again, the hostility, the aggression. And, and so that happened in the sixties. And again, documented really well in the, in the book The Protests Psychosis, but that happened in the 60s. But what we have here in modern times, which has been really well studied by many researchers and could, including Steve Strakowski is that we see inequities in all sorts of outcomes, as it relates to, um, people of color and Black people and schizophrenia.
So Black people are more likely to be diagnosed with schizophrenia than with a mood disorder, like bipolar disorder or depression compared to white people. And, um, they're, they're, they're misdiagnosed, so they may have bipolar disorder and they're misdiagnosed as schizophrenia.
[00:40:08] Anne: Can you help me, um, I guess, understand the differences between these two diagnoses and kind of, yeah, understand the differences in why it matters if you're given one, versus the other, like with one student
[00:40:21] Ruth: matters a lot because of treatment options. And so when you have a mood condition, the treatment is a mood disorder. The treatment is often very different from a primary psychotic disorder.
And so, um, if you don't, if you're misdiagnosing the condition, you're often then providing the wrong treatment. Um, and so if somebody is not getting the most effective treatment for their condition, then they're not going to improve. And so, so what you see is in this particular population, a misdiagnosis followed by then, um, not the right, uh, management of symptoms, so a lack of improvement and then, um, you see these populations having again, worse outcomes.
So, so if you have misdiagnosed Black people, um, at higher rates, then those people do not recover completely from their illnesses. And then we look at like rates of, of, um, treatment responsiveness. And we say this particular population does not respond as well to this particular medicine or this particular therapy when really what it came down to was that the diagnosis was wrong in the first place.
Um, but even beyond making a mistake in the diagnosis, um, we also see things like, again, associated with this, this conceptualization of aggression, we see things like Black people are more likely to be put in seclusion and restraints. Um, when they go to the hospital for emergency psychiatric care, they're more likely so they're more likely to be seen as hostile and aggressive. They're more likely to be given, um, antipsychotic medications against their will to manage their behavior. Um, and they're more likely to be given higher doses of those antipsychotic medications. So, so the management, uh, in addition to the misdiagnosis, the management in crisis situations is, is more harmful.
Um, and like a very clear example I can give you is from my personal, um, clinical experience I've had, um, there, there are many different medications that you can use to treat psychotic symptoms. But one of the medications, an older medicine haloperidol is a medication that back in the 60s, um, when they were, uh, very strongly associating Black people with aggression and psychosis and schizophrenia, um, there were ads that you started to see, um, pop up in, um, psychiatric journals, which showed like a threatening aggressive Black man, um, and, and the, the headline on that ad the tagline on that ad set aggressive belligerent cooperation begins with Haldol. Um, and so what you've seen over time is that that particular medication somehow became associated in the minds of psychiatrists with that direct marketing with, oh, this is the medication you use when some, when a Black person presents with schizophrenia and is aggressive.
And so that marketing was very effective because, um, last year, one of my patients had to go into the hospital. Um, and I have, I have him on an antipsychotic medication and he was doing reasonably well, but then he had a, uh, a decline in his functioning. Um, and he went into the hospital and, um, he was hospitalized in a psychiatric facility.
And the first thing that the inpatient psychiatrist did was remove him from his medicine and start him on Haldol. And I thought to myself, why, why would, would that be the choice, the first choice, you know, and I, I certainly don't want to imply, um, that, that this, this inpatient psychiatrist was racist. Um, but I, but I also think there was a clear connection there because there is this connection in this drug that this drug works in this particular population.
It would be fine if that was a one-off thing, but a year later, uh, another patient of mine who is a Black woman, also went into the hospital because she had a decline in her functioning and she was taken off of her medication and put on Haldol. Now that being said, I have several white patients that when they go into the hospital, they are not put on Haldol.
So, so even today we see these inequities kind of, uh, and, and, and, you know, it's complicated because it's not like Haldol is a terrible medication. Um, but it has side effects and it has, and there are things to be considered, and it's not first-line anymore, really all the time for like ongoing outpatient management of schizophrenia.
And yet the only times that I've seen inpatient doctors prescribe that medication, um, to my patients is when they are, um, deemed to be aggressive or threatening or are, or when they're Black.
[00:45:28] Anne: Wow. Even today, it's like, it's not surprising and yet it's still
[00:45:35] Ruth: shocking. Even, even when it's not surprising, it's still shocking.
Anne: Yeah. Yeah. That's a really good distinction.
[00:45:46] Anne: So looking beyond like, these are heinous things to happen to individuals, but when you're treating individuals are not just looking at an individual, you've got a whole family and a whole community. How, how did these, um, how do these beliefs then spiral out wider into communities?
[00:46:08] Ruth: Um, I think that, I think that we, part of what happens is, as, so we, we are not, we are, we, human beings are not islands. And so we do not operate, um, independently. We operate within our family units. We operate within, um, our communities. Um, and I think that when one person has a negative interaction with the mental health um, system that scars families and communities.
Um, and, and, and again, um, so, so we know that, and I know from personal experience, you know, if you experienced discrimination, if you experienced mistreatment, when you go for, uh, services or care somewhere, um, I have never returned to a restaurant that I ate at where I felt I was discriminated against.
I've never once been like, okay, I'll go back there because it was probably a one-time. I always think I have choices, I have options, and I don't need to go to that restaurant again. Um, and so for mental health care, it's a little bit different. Um, people go and they're mistreated and they may be discriminated against in healthcare settings, um, and they then have very limited options about like, how, how do they re interface with that, um, with that setting. And so the damage that can be done, the damage that's done to one person, um, then ripples through that family. And so I spend a lot of time interacting clinically with family members who have been traumatized by watching their loved ones, be harmed, um, in seeking care, or be made to feel less than, or be, or be discriminated against in their pursuit of mental health care at maybe some of the worst times in that family's life when, when someone is in crisis and they need help and they're made to feel less than, and they're made to feel, um, not important and not valuable. Um, and so that then is, causes a ripple effect and then the whole family, um, and the whole community tends to kind of turn away from seeking those services.
And so that's when you end up with this narrative that certain populations, certain racial and ethnic groups, Black and Latinx populations, for example, indigenous populations that they, um, have so much stigma that they don't want to interact with the mental health system. And I'm not saying that stigma doesn't exist and I'm certainly not saying, um, no, there is no stigma, but I actually don't think that the driving factor in minoritized populations or populations that have traditionally been oppressed, I don't think it's actually stigma.
I think it's a very reasonable response to a system that has been harming individuals and a desire not to willingly interface with a system that has, that treats you like you're not worthy or is more likely to put you in seclusion and restraints when you go for crisis help. You know, I think that it's a very reasonable thing, not to want to interact with that system.
So it's not a stigma problem, as much as it's, uh, a general reasonable response to a trauma being elicited on you. And so then the, the, it's really important because the intervention is very different. So many times people say, oh, there's stigma in these particular populations. So we have to educate people on how important it is for them to seek mental health services and how important, and that is not where the emphasis needs to be.
The emphasis needs to be on us, improving the mental health system and to be providing, um, culturally humble services and structurally competent and structurally humble services that values and appreciates people and makes them feel, um, important and, and cared for. Um, and if we fix the system to be more trustworthy, then people will engage with the system more.
So it's not about educating. Um, it's not about educating certain populations and say, oh, you know, come, come to our health care system. If the onus is on the providers and the people in the healthcare system to make it a better place for people to enter.
[00:50:35] Anne: And you, you've done some work trying, like, talking about specific ways that could happen. What are specific ways? Like what, how can we make the mental health care treatment system actually responsive to people in a more inclusive? Not my, I hate the word inclusive,
[00:50:53] Ruth: I like the word inclusive.
[00:50:58] Anne: I think, I feel like I've encountered, oftentimes people are like, oh, let's make it inclusive, but they don't really,
[00:51:04] Ruth: there is no action following the inclusivity. Yeah, I hear you.
[00:51:09] Anne: So that's, I guess that's what I mean, like how do we make it like actually inclusive and mean it?
[00:51:16] Ruth: So I, I feel, I think there's many ways and I, um, but I, but I think that the lack of inclusivity and real action behind that inclusivity has to do mostly with power and power dynamics and who has power and who doesn't.
And so if we start to kind of like tease that apart, we see systems that are designed, um, to make it clear when people interface with those systems, that the people who have power are powerful, um, and that the people who don't are made to feel less than. And so then the work becomes unraveling that hierarchy that we have created within our mental health systems.
And that can happen on multiple levels. But I think the quickest way, the quickest way to get there is to have the people working in that system, be the very people, be the very people who are actively, um, from those communities and members of those communities.
That's when workforce diversity becomes most important because, um, because that is not the traditional ways that mental health clinics are designed. the mental health clinics do not traditionally reflect the demographics of the population that they're serving.
And so it, it really does. So it's not just a matter of, um, of, of creating a more diverse workforce. It's truly having the people that work in that particular mental health setting be from the very community that they're serving and look, and be those members of that community. And this is one of the reasons why I am so kind of supportive of the idea of peer specialists, because it is, it is, that is the very function of, of a peer specialist to be a person from the community who has lived experience, who knows exactly what it feels like to go through this situation and to be able to provide that care and support.
And that is the fastest way that we will make the settings, um, we, we will redesign these settings so that people can come in and feel valued and feel important because they are the setting. They are the people that are in that setting. And so that's the work that we have to do. Um, and that involves across all levels, um, aggressively diversifying the workforce.
Um, and we talk about workforce shortages and all of that, but I think we need more psychiatrists of color. We need more psychiatrists from oppressed and marginalized backgrounds. We need more sociologists and social workers and psychologists and peer specialists from, from all sorts of backgrounds.
Um, and that is the way that we, um, change, change the system and, and truly build an inclusive, um, mental health system.
[00:54:16] Anne: I'd like to delve a little bit more into, um, you kinda touched on people's lived experience and bringing that in and, and social determinants of health. Um, I'd love to kind of talk more about what can be done or what you're advocating people within the mental health field to do to really account for all of these other factors that influence our mental health, as opposed to just seeing a therapist or a psychiatrist.
[00:54:47] Ruth: I think one of the best ways that people can start to take action is by increasing awareness.
Um, and, and so I think that the mental health field, as it's kind of currently structured, spends a lot of time thinking about the individual patient that sits in front of, comes to the office and sits down in front of them. Um, and does an assessment that again, doesn't have all of the context in place and particularly the context that I think most providers miss when they do an evaluation on a, on a client or a person with a mental health problem is that they're missing the structural components.
They're missing that understanding of how those social determinants are interacting directly with that individual. So they're not understanding how, um, access to healthy foods or how poverty or how adverse childhood experiences or how homelessness or housing instability, um, they're not always understanding, uh, or how discrimination and racism and sexism, how they're not always understanding how those things show up in people's lives and they're not searching for it.
They're not asking questions about that. So they're not asking people about their identities. They're not trying to understand like who this person is and how the external world, um, has, has interacted with that person and who they are and who their identity is. Um, and I think that, uh, if, if we, as providers don't do that work, um, we're, we're dropping the ball on, on taking care of whole people and moving them towards health and wellness.
So, so the, the key, um, and the first step is recognizing that when somebody comes and sits in front of you, um, for an evaluation or for help, and, uh, in managing their mental health, that they're not just some diagnosis or they're not just some condition, but they are like a whole person who brings multiple identities and multiple, um, beliefs and, and, and multiple cultural, um, cultural identities to, to who they are and that, and that the job of the provider is to understand better that person's story and how they interact with the world and how the world interacts with that person.
So some people talk about this in the concept of structural competence. And this is again, um, Jonathan Metzl and Helena Hansen. This is work by Jonathan Metzl and Helena Hansen, um, to think about how we talk about cultural competence. We, we, we talk about how it's important to understand that there are lots of different cultures and understand the groups, um, that different cultures have different values.
But part of what structural competency is saying is we have to better understand how all of those social determinants show up in people's lives. And we have to be better at identifying those social determinants and asking people about those social determinants and thinking about that context.
[00:58:05] Anne: So to put this into terms that aren't using, like structural competency or social determinants, like basically helping providers, but potentially also helping individuals understand like all of the different factors that are happening around them and how that influences them from the stress of not having enough food to the stress of being discriminated against to the stress of having to navigate complicated systems that weren't built for you to navigate.
[00:58:39] Ruth: Exactly. Exactly.
[00:58:43] Anne: Making sure that I could explain this the way it's supposed to be. Explain it's it's
[00:58:46] Ruth: You explained it beautifully. And I think, um, that, that that's the key is, is that's not the model by which most psychiatrists are trained. Psychiatrists are trained to say, what are your symptoms? Um, you know, how much have you, you know, what's your appetite been like?
So like ask about appetite because appetite is a symptom of depression and poor appetite is a symptom of depression. Um, so ask if your appetite has changed, but not ask how, how, how easily can you access food? How easily can you access healthy foods? Um, do you have food insecurity?
And so there's like a number of the symptoms. So, uh, lack of sleep is, um, another symptom of depression. And so we ask those questions, how's your sleep, but we don't ask, um, is there like noise in your neighborhood that prevents you from sleeping? Is there, um, you know, are you witnessing violence or are you experiencing things that are interfering with your sleep that aren't just, I have this symptom of, of insomnia.
So it's really about it's, it's about going deeper and understanding how those environmental factors really do, um, come into play when, and we are social beings that interact with our environment. It seems pretty obvious, right?
Like we should be assessing how people interact with their environments and what's in those environments. Um, and that is just as critical as just understanding and ticking off the symptoms of certain disorders and conditions.
[01:00:19] Anne: This is going to sound like, like a really basic question, but I would love it if you could talk about, even just really quickly, like how discrimination directly affects mental health. Um, just so that people like grasp that.
[01:00:34] Ruth: Yeah. That's not a basic question at all. Um, uh, it's, it's a great, it's a great question. When, um, when I was working on, um, the book, the book, I edited, The Social Determinants of Mental Health, we were, um, trying to gather all those determinants and look at their impact on mental health outcomes. And there was this really fascinating pattern that we were just, uh, noticing when we were writing that book because we looked at things like discrimination, we looked at housing, we looked at food, we looked at adverse childhood experiences and there wasn't a lot of data out there at the time. And one of the things we noticed is that there was, um, a lot of data that showed, um, for almost all of those social determinants, there was a lot of data that showed, uh, that people, um, have significant physical health problems associated with things like adverse childhood experiences and housing instability and food insecurity.
Um, and there was less data to support that there were mental health impacts. We found them, but they were harder to find. And it was like that for all of the social determinants except discrimination. So for discrimination, there was not a lot of evidence to show that discrimination directly led to poor physical health, but there was an abundance of information and lots of data that showed that discrimination leads to poor mental health outcomes.
And specifically, certain diagnoses are directly correlated with being perceived as being discriminated against. So you actually don't even have to have been actively discriminated against. You, just as an individual, have to feel as if you were discriminated against. And that would lead to an increased risk of a number of mental health conditions, including major depressive disorder, alcohol use disorder, post-traumatic stress disorder, more days of having psychological distress, um, all of those illnesses, um, and all of those mental health conditions are tied directly to the experience of perceiving that you are discriminated against.
And so there's a direct line there. And again, it's really powerful because, um, that data is, is really robust data that we have on this. So absolutely discrimination leads to poor mental health and leads to poor mental health outcomes. And we have really strong data that scientists have been working on for, for decades now that that says that pretty definitively.
[01:03:15] Anne: And so the solution for that is?
[01:03:21] Ruth: Less discrimination. Less discrimination, I think is the key. How do we eliminate discrimination? Um, and, and so, you know, that, that leads a lot of people to say, okay, that's where we have to do implicit bias training. And I do think implicit bias training is one piece, but, but I also, again, I'm back to at least, you know, we can't solve discrimination in the world, you know, like that's too big of a, uh, a thing to address, but we can at least minimize the discrimination that people experience accessing healthcare.
Um, and there is, you know, um, David Williams is a researcher on, on racism and discrimination and health, and he created an everyday discrimination scale. And this is like a scale that asks people how they've been discriminated against in, in, in their lives. And this is where a lot of that data comes from that shows that if you score higher on that everyday discrimination scale, you have a greater likelihood of developing, um, a number of mental health conditions.
And, and one of the things that, uh, happened is that that everyday discrimination scale was adapted for health care settings. And so the same questions are now asked, has a nurse or doctor ever made you feel, um, that you were less than, or talk to you? Like you were, um, not important or, you know, made you feel like you were stupid.
Like those questions, um, that were part of the regular scale have now been adapted for the healthcare setting. So we can't fix all of the ills of society, but we could at least eliminate the discrimination that people experience when they go to seek health care and the discrimination that they experience when they get mental health care services.
And, and again, one of the quickest ways we can do that is by diversifying the workforce, by making sure that there are more people from those same identities providing care, because it's less likely that somebody is going to be discriminated against, by someone from the same group or category that they are in.
[01:05:25] Anne: Anything else you'd like to add before you run to your next meeting?
[01:05:29] Ruth: No, I just thank you so much for the time. It's been great to talk to you.
[01:05:33] Anne: Likewise. Thank you so much for your time.
That was Dr. Ruth Shim talking about racism and mental health. As Dr. Shim said, there are ways to make the mental health system more equitable. Part of that starts with diversifying the workforce and valuing the skills and life experiences that peer navigators bring to the table. Providers also need to consider all of the different aspects of life that influence our mental health, like the resources we have access to and the environment we live in.
During the next full episode of Mental Health Mosaics we'll delve more deeply into another issue that influences our mental health -- our sense of identity. You can find more resources related to all of these issues as well as poetry and art on our website, mental health mosaics -dot- org. If you enjoyed today's episode, help others find it by rating the podcast on any and all podcast platforms.
Today's episode was edited by Susy Buchanan with audio editing by Dave Waldron. Our theme music is by Aria Philips. I'm the show's host and producer. We received funding from the Alaska Center for Excellence in Journalism, the Alaska Mental Health Trust Authority, and the Alaska State Council for the Arts.
Thank you for listening!
White Supremacy Culture
White supremacy culture
White supremacy culture is suffused in all aspects of life in the United States, from the belief that any individual can get ahead to either/or thinking.
All of this is laid out on a website by Tema Okun anted is derived from her widely circulated 1999 essay. The website isn't mobile-friendly, so you can read most of her points on this PDF.
The Vu Le at Nonprofit AF has a list of ways the white supremacy sneaks its way into nonprofit work, through mostly white leaders to taking feedback mostly from white funders. This really applies to many types of work, not just nonprofits.
Many other resources, from discussions of "professionalism" to examining workplaces values, are on Racial Equity Tools.
The use of the term white supremacy outside of the context of hate groups like the KKK and neo-Nazi is controversial, as discussed in this New York Times article from 2020.
All of this is laid out on a website by Tema Okun anted is derived from her widely circulated 1999 essay. The website isn't mobile-friendly, so you can read most of her points on this PDF.
The Vu Le at Nonprofit AF has a list of ways the white supremacy sneaks its way into nonprofit work, through mostly white leaders to taking feedback mostly from white funders. This really applies to many types of work, not just nonprofits.
Many other resources, from discussions of "professionalism" to examining workplaces values, are on Racial Equity Tools.
The use of the term white supremacy outside of the context of hate groups like the KKK and neo-Nazi is controversial, as discussed in this New York Times article from 2020.
Other Important Links
Other important links
|
Subscribe to the Mental Health Mosaics podcast!
Subscribe to the podcast!
Subscribe!
